
Highlights
- • A combination of (i) an incentive motivation model of sex and (ii) dual control theory is presented.
- • By the criteria of (i) suffering and (ii) a shift in weight of control from goal-based to stimulus-based, sex can become addictive.
- • Scrutiny of the criticisms of the notion of sex as addiction reveals them to be invalid.
- • Similarities between sex addiction and drug addiction are noted.
- • Out-of-control sexual behavior is not best characterized as hypersexuality, high drive or an impulse control disorder.
Abstract
An integrative model of sexual addiction is presented, involving a combination of models based upon (i) incentive motivation theory and (ii) the dual organisation of the control of behavior. The model is related to ongoing arguments about the validity of the notion of addiction when applied to sexual behavior. It is suggested that the evidence strongly favors the viability of an addiction model of sex. Strong similarities to the classical addiction to hard drugs are observed and features can be better understood with the help of the model. These include tolerance, escalation and withdrawal symptoms. It is argued that other candidates for accounting for the phenomena, such as obsessive-compulsive behavior, faulty impulse control, high drive and hypersexuality do not fit the evidence. The role of dopamine is central to the model. The model’s relevance to stress, abuse, development, psychopathy, fantasy, sex differences, evolutionary psychology and the interaction with drug-taking is shown.
1. Introduction
Since its formulation by Patrick Carnes in the early 1980 s (Carnes, 2001) the notion of sex addiction (SA) has garnered considerable support and provided explanatory insight (Birchard and Benfield, 2018, Firoozikhojastehfar et al., 2021, Garcia and Thibaut, 2010, Kasl, 1989, Love et al., 2015, Park et al., 2016, Schneider, 1991, Schneider, 1994, Sunderwirth et al., 1996, Wilson, 2017). Sexual addiction is usually compared with drug addiction and some striking similarities noted (Orford, 1978).
Despite wide acceptance of the notion of sexual addiction, some prefer to wait-and-see before a full commitment to the term (as indexed by considerations for inclusion in DSM-5) Others see virtue in both addiction and obsessive-compulsive models to explain ‘out-of-control’ sexuality (Shaffer, 1994). Finally, there are also uncompromising sceptics, presenting their critiques of the notion of sexual addiction in the academic literature (Irvine, 1995, Ley, 2018, Prause et al., 2017) and in popular books (Ley, 2012, Neves, 2021).
The theoretical framework adopted in the present study is a combination of models based upon (i) incentive motivation theory and (ii) the dual-control organization of brain and behavior, each of which is introduced shortly. The central theme advanced is that the potentially addictive nature of sex and the similarities between sex and drug addiction can be more clearly appreciated when viewed in terms of an up-to-date motivation theory. The present article rests fundamentally on the criteria that addiction is suggested where there is:
- • suffering and a wish to be free of the excessive behavior (Heather, 2020).
- • a particular set of learning mechanisms and causal processes involved (Perales et al., 2020) (Section 2).
The model proposed also allows integration with an evolutionary perspective on addiction.
Some draw a distinction between pornography addiction and addiction to sexual behavior, suggesting that the former can be a subset of internet addiction (Adams and Love, 2018). The present article takes a broad brush-stroke approach in grouping together addiction to sexual behavior and pornography.
Much evidence has been gathered to favor a dual-systems model of behavior (Pool & Sander, 2019; Strack and Deutsch, 2004), including sexual behavior (Toates, 2009, Toates, 2014). However, only recently has the dual systems notion been applied in depth to behavioral addictions (i.e. non-drug related) (Perales et al., 2020). Although there are occasional references to the relevance of dual systems models to sexual addiction (Garner et al., 2020, Reid et al., 2015), there has so far been no integrative review of the topic. The present paper develops the dual model in the context of an integrative review of sexual addiction.
2. Characterizing the processes underlying motivation
Two basic dichotomies can be drawn, as follows (Table 1). As the first, there is a dual structure in the control of behavior, i.e. stimulus based and goal based. This can be mapped onto the distinction made by Perales et al. (2020)between compulsive (stimulus based) and goal-driven (goal based). As the second dichotomy, in addition to excitation, there are corresponding processes of inhibition, also organized in a dual structure.
Table 1. Processes underlying motivation.
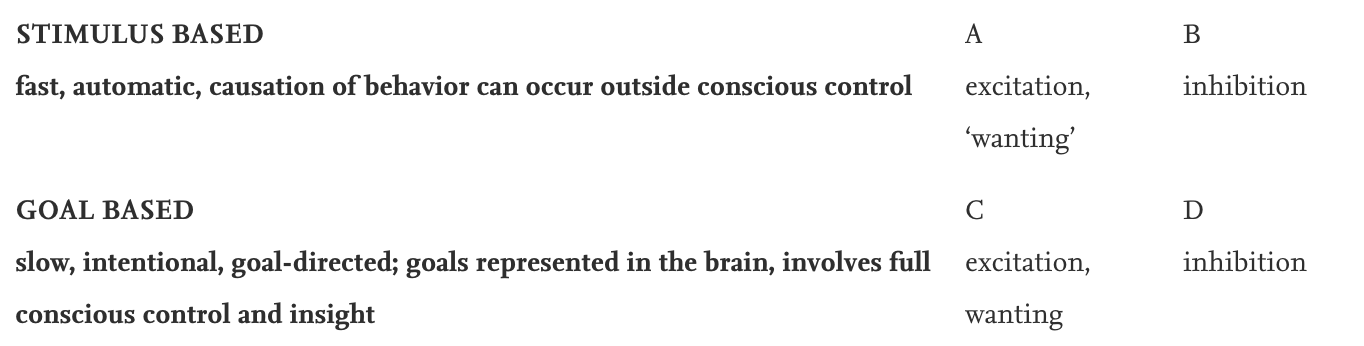
In the case of addiction, stimulus-based control has two components, as follows. A well-known statement of the idea of dual control is that of Kahneman (2011): a fast, automatic System 1 that can act outside conscious awareness and a slow goal-directed System 2 that acts with full conscious awareness. This distinction refers to the control of behavior and thought. It applies throughout much, if not all, of the control of behavior, including addiction. With repeated experience under a given set of conditions, behavior becomes more habit-based, e.g. the mechanical actions involved in using a drug or the routes taken to acquire a drug (Tiffany, 1990).
The second aspect of this stimulus-based mode of control is peculiar to motivational processes and in particular addiction: the targets of behavior acquire increased power (‘magnet-like’) to lure the addicted person (Pool & Sander, 2019; Robinson and Berridge, 1993).
The discussion proceeds with a further consideration of Box A in Table 1. It occupies a disproportionate amount of space here, since it has been the principal focus of theories of addiction.
3. Incentive motivation
3.1. Basics
Central to motivation research is the incentive-motivation model (Ågmo and Laan, 2022, Bindra, 1978, Robinson and Berridge, 1993, Toates, 1986, Toates, 2009), approach motivation being triggered by:
- •
-
particular incentives in the external world, e.g. food, drugs, a potential sexual partner.
- •
-
cues associated with such incentives, e.g. a classically conditioned association between the keyboard on a computer and the appearance of pornographic images on the screen.
- •
-
internal representations of these incentives in memory.
Robinson and Berridge’s (1993) incentive motivation theory of drug taking and addiction provides a massively influential account. The authors acknowledge its relevance to the so-called behavioural addictions, such as sex (Berridge and Robinson, 2016) and it forms a foundation of the present article.
3.2. A response bias
The term ‘cue reactivity’ refers to the activation of a collection of brain regions in response to cues such as the sight of drugs or those predictive of drug availability. The notion is also applicable to sexuality, i.e. a relatively high reaction to sexual cues, as shown, for example, by men with a problematic use of pornography (Kraus et al., 2016, Voon et al., 2014).
A tendency for addicted people to show a bias of approach towards the target of their addiction has been extensively investigated in a range of addictions, substance-related and non-substance related. For sex and drugs, the stimulus-based control can act at an unconscious level before the on-going approach reaction enters conscious awareness (Childress et al., 2008). For this reason the word wanting in Table 1 Box A is represented as ‘wanting’, to distinguish it from conscious wanting. The magnitude of the approach bias towards erotic cues is higher in males (Sklenarik et al., 2019) and females (Sklenarik et al., 2020) with problematic pornography use.
3.3. Wanting and liking
A feature revealed by drug addiction is a separation of wanting (encompassing both senses of the term) and liking (Robinson and Berridge, 1993). After extensive use, a drug might be wanted intensely without there being a commensurate liking of it once taken.
Although wanting and liking are distinct processes, they are strongly interactive. That is, incentives are calibrated based on the consequences of interaction with them. Indeed, it would be a strange ‘design’ if things were otherwise. We normally like what we want and want what we like, even though these processes can slip into misalignment (Robinson and Berridge, 1993).
Voon et al. (2014) reported a dissociation whereby a high value of wanting in problematic pornography users was not associated with a correspondingly high liking. Intense sexual wanting can co-exist with little or no liking (Timms and Connors, 1992). Ironically, the occasional individual reports sexual pleasure with a regular partner but not derived from extra-pair addictive activity (Gold and Heffner, 1998). In one sample, 51% reported that over time their sexually addictive activity got less pleasurable or even that they derived no pleasure from it (Wines, 1997). Two sexually-addicted patients, reported that early delight with sex gave way to disgust in adulthood (Giugliano, 2008, p146). Doidge (2007, p.107) reported:
“Paradoxically, the male patients I worked with often craved pornography but didn’t like it.”
3.4. Biological bases
Sescousse et al. (2013) identified a common brain network that is activated by such rewards as food, sex and monetary stimuli. This network involves the ventromedial prefrontal cortex, ventral striatum, amygdala and anterior insula. At center-stage in discussions of incentive motivation is the pathway of dopaminergic neurons projecting from the ventral tegmental area (VTA) to the ventral striatum, more specifically the striatal region known as the nucleus accumbens (N.Acc.) (Robinson and Berridge, 1993).
Activity in this pathway underlies wanting but not liking. Rather, liking is under the control of other substances, most clearly opioids. Repeated activation of this pathway leads to what Robinson and Berridge term ‘incentive sensitization’, i.e. the capacity of drugs to trigger this pathway becomes sensitized. The salience of the drug is increased. Evidence suggests that repeated excitation by sexual stimuli can have a similar effect (Lynch and Ryan, 2020, Mahler and Berridge, 2012).
Voon et al. (2014) found that men with problematic pornography use showed higher reactivity to sexual cues in a collection of brain regions: the dorsal anterior cingulate cortex, ventral striatum and amygdala. This was relative to men who were able to view without problems. Using fMRI, Gola et al. (2017)found that men with problematic pornography use showed elevated reactivity in the ventral striatum specifically to cues predictive of erotic images but not to those predictive of monetary images (see also Kowalewska et al., 2018 and Stark et al., 2018). They did not respond differently to controls in reaction to the actual images. The men with problematic viewing expressed strong wanting of the erotic images but appeared not to like them any more than did a control group without problematic pornography use. Similarly, Liberg et al. (2022) showed that those with a problematic use of pornography exhibited a heightened reaction in the ventral striatum to the anticipation oferotic images, a response that correlated with how much they reported looking forward to seeing the erotic images. Demos et al. (2012) found that the reaction of the nucleus accumbens to erotic images was predictive of subsequent sexual activity, while the reaction to food cues predicted future obesity.
Activity in this pathway is particularly sensitive to novelty and uncertainty of reward, something researched extensively in gambling (Robinson et al., 2015). These must surely be highly potent features of those erotic stimuli to which people become addicted, e.g. the limitless range of pornographic images, the variety of sex workers offering their services.
The addictive potential of a drug depends upon the speed with which it gets to the brain following taking it and the intermittency of use (Allain et al., 2015). By comparison, information on visual stimuli often arrives at the brain very rapidly following exposure, e.g. a click on the keyboard and pornographic image appearing, or images might even arise in the imagination. Also sexual incentives are commonly encountered intermittently and with uncertainty, as in the searching for and use of sex workers.
Activation of opioidergic transmission corresponding to liking tends to increase dopamine activation in response to the incentive being encountered subsequently (Mahler and Berridge, 2009).
Ley (2012, p.101) makes the correct observation that the brain is constantly changing in response to changing life events, e.g. to learn a new language or to ride a bicycle. From this, he concludes that brain changes associated with sexuality are no more significant than those associated with any other activity. This is misleading since some of the brain changes underlying addiction are within specific motivation pathways, e.g. dopaminergic systems and the pathways that synapse upon them (Section 3.4).
Smith (2018a, p.157) writes:
“……the changes in the brain that take place as addiction grows are the same as changes that take place as any habit develops.”
The changes with, for example, learning to brush teeth or ride a bicycle are in regions concerned with eye-hand coordination and motor control. Unlike with addictions, these habits do not thereby acquire ever-increasing motivational urge over time.
There are rich opportunities for classical conditioning to occur in sexual addiction, e.g. the computer keyboard associated with viewing pornography can provide excitation (Carnes, 2001). Presumably, by analogy with drug addiction, as a biological basis this has the excitation of dopaminergic neurotransmission by conditional stimuli.
3.5. Formation of incentives
Sexually addicted people often acquire special targets of desire (Carnes, 2001), a kind of imprinting. For example, some people addicted to cybersexdescribe particularly potent images as being “burned-in” to their minds (Carnes, 2001). Amongst some of these images, there exists a process of reversal of polarity from aversive to appetitive (McGuire et al., 1964), e.g. forced exposure of a young boy’s genitals in childhood is followed by adult exhibitionism (This appears to have features in common with the opponent-process model of Solomon, 1980). It seems that high arousal is the common factor through changes from aversion to appetitive (Dutton and Aron, 1974).
4. The controls located in Boxes B-D
4.1. Basics
The system of behavioral control just described forms the principal focus of investigations into addiction (Box A). This section turns to those described in boxes B-D of Table 1.
4.2. Goal-based excitation
The ‘goal-based control of behavior’ (Box C of Table 1) describes that associated with full conscious processing (Berridge, 2001). In the context of addiction, the goal is based upon the hedonic representation of the reward in the brain (Perales et al., 2020). This involves the ventromedial prefrontal cortex (Perales et al., 2020) and is at the basis of wanting, with no inverted commas. It exerts inhibition on any tendencies that are incompatible with the goal (Stuss and Benson, 1984, Norman and Shallice, 1986). Prior to 2001, details of the dual processes were to be found in entirely distinct literatures, thereby missing the issue of how they control behavior in interaction. Berridge (2001) brought both processes under one roof in an integrative review.
5. Inhibition
5.1. Basics
There are processes of active inhibition on sexual desire and behavior (Janssen and Bancroft, 2007). That is, loss of desire is due not just to a loss of excitation but also to inhibition that opposes excitation, a form of tug-of-war. As with excitation, inhibition is represented by dual controls (Berridge and Kringelbach, 2008, Hester et al., 2010, LeDoux, 2000).
One type of conflict that can arise is when resisting temptation, the pull of an incentive (Box A) being pitted against the goal (Box D). Conversely, a person sometimes needs to overcome a reluctance generated by an aversive stimulus, as in eating a badly-tasting food in order to please a host (Box C).
5.2. Relevance of inhibition to sex addiction
Janssen and Bancroft (2007) described 2 types of inhibition on sexual behavior: due to fear of (i) performance failure and (ii) performance consequences. Toates (2009) fitted this to the notion of dual control, with Janssen and Bancroft’s ‘fear of performance failure’ corresponding to stimulus-driven inhibition (e.g. a loud sound, foul odor, perception of erectile difficulty) (Box B), and ‘fear of performance consequences’ corresponding to goal-directed inhibition (e.g. a wish to retain fidelity) (Box D).
In keeping with a broad perspective on the role of dopamine and serotonin, Briken (2020), Kafka (2010) and Reid et al. (2015) suggest that these neurotransmitters are involved in excitation and inhibition respectively.
6. Interactions and weightings between controls
Although there are two modes of control, they are strongly interactive. Any given piece of behavior could be understood as being somewhere on a continuum in the weight of control between the two (Perales et al., 2020). The relative weight of the controls changes with various circumstances.
6.1. Facing temptation and giving in to it
When facing temptation and resisting it, the assumption is that the fully conscious system (Box D) inhibits tendencies to act. As the incentive is approached, so the strength of temptation increases. As a qualifier to this broad assumption, there are times when activity within systems of conscious control can assist in giving in to temptation, a phenomenon described by Hall (2019, p.54) as “cognition distortion”. This is where it concerns silent messages to oneself of the kind “this one time won’t matter” (Kasl, 1989, p.20; Vigorito and Braun-Harvey, 2018).
6.2. Arousal
With high arousal, behavior becomes more stimulus-based and impulsive, while restraints exerted from conscious cognitive decision-making carry less weight. This principle has been applied to sexual risk-taking (Bancroft et al., 2003) and is described by the term ‘heat-of-the-moment’ (Ariely and Loewenstein, 2006). Evidence points to sexually addicted people showing such a shift of weight. Reid et al. (p.4) describe sexual addiction as:
“……a failure in “top-down” cortical control of frontostriatial circuits, or from overactivation of striatal circuitry”.
Ley (2018, p.441) states that.
“….neuropsychological testing reveals that sex addicts demonstrate no measurable problems in impulse control and executive functioning.”
This is true in the study cited but that was done in the context of performing the somewhat emotionally-cold Wisconsin Card Sorting Task. Reid et al. (2011) make the point that their results might well not generalize to a situation of sexual temptation.
6.3. Repeated experience
Some parts of the control of behavior become more automatic with repeated experience. Such a shift, based upon increasing incentive salience, represents a criterion for the definition of addiction (Perales et al., 2020). On out-of-control sexual behavior, Hunter (1995, p.60) writes:
“By the time someone has developed a psychological addiction to an act, it has taken on a life of its own. The actions are so automatic that the addict will report that they “just happen” as if he or she played no part in the action.”
A move to automaticity corresponds to increased weight of control taken by the dorsal striatum relative to the ventral striatum (Everitt & Robbins, 2005; Pierce and Vanderschuren, 2010). However, control does not shift entirely to automatic mode (Section 15.3).
7. Fantasy
Fantasy is of crucial importance in sex addiction. A favoured image acquired early can accompany masturbation or partnered sex (reviewed by Toates, 2014). It appears that, given appropriate circumstances, repeated fantasy can strengthen the tendency to enact it in behavior, (Rossegger et al., 2021). A therapeutic technique in forensic cases involves trying to satiate or devalue the fantasy (Rossegger et al., 2021).
Some of the same brain regions that are excited by the sight of drugs are also excited by thoughts of them, associated with craving (Kilts et al., 2001) Therefore, it seems reasonable to extrapolate and suppose that fantasy can excite incentive motivation processes underlying sexual desire.
8. Regulation and control
The literature assumes that sexually-addictive behavior, as with drug addiction, serves a regulatory function, i.e. to regulate mood (Katehakis, 2018, Smith, 2018b), a form of homeostasis. This has echoes of John Bowlby (Bowlby and Ainsworth, 2013). Under optimal conditions for the non-addicted individual, mood is maintained by social interactions with family and friends, a manifestation of belonging (Baumeister and Leary, 1995).
In many cases of addictive behavior, something has often gone wrong with the process of attachment and so addictive behavior serves as a substitute. Translating this to the underlying biology, evidence points to regulation being based upon endogenous opioid levels (Panksepp, 2004). When these fall below optimum, control action is taken to restore normality. This control action is rooted in dopamine (Section 3.4). By analogy, body temperature is regulated with the help of controls over such things as sweating, shivering and behavior motivated to seek a different environment.
9. Epidemiology
Some 80% of people with SA are male (Black, 1998). Men are more likely than women to engage in bought sex, pornography and paraphilias such as exhibitionism and voyeurism, whereas women are more likely than men to give a shade of love addiction to their SA (Black, 1998). In one sample of SA, relative figures for number of sex partners in the previous 5 years was 59 (men) and 8 (women) (Black, 1998).
10. Evolutionary arguments
10.1. Normal stimuli and supernormal stimuli
The environment in which we evolved was radically different from today’s environment, which contains an abundance of pornography and readily-available sex. The term ‘supernormal stimuli’ (Tinbergen, 1951) captures this feature of our present sexual environment (Adams and Love, 2018).
By the same logic, clearly casinos and on-line betting are recent cultural inventions which lock onto those mechanisms that evolved to produce persistence in the face of scarce resources. Similarly, an abundance of easily-available sugar-laden foods characteristic of affluent cultures were not part of our early evolution. This is reflected in food addiction and obesity. In incentive motivation terms, contemporary environments present easily accessible incentives which are vastly more potent than those of the environment of early evolutionary adaptation.
10.2. Sex differences
In response to erotic stimuli, the amygdala and hypothalamus show a stronger response in men than in women (Hamann et al., 2004). The authors suggested that this could correspond to a greater appetitive incentive value of erotic stimuli in males.
Women are more likely to be addicted to love rather than to sex per se, whereas for the male the tendency is to pure sex addiction (Katehakis, 2018). The female addiction can be manifest in an endless series of romantic relationships. Under normal conditions, sexual desire in women is more often contextualized in terms of meanings (e.g. does he value me as a partner?), whereas male erotic desire is more strongly driven by attractive features per se (Toates, 2020). Addictive sex appears to represent an exaggeration of this sex difference.
The expression ‘Coolidge Effect’ refers to the arousal value of novelty in sexual behavior (Dewsbury, 1981). Clearly, this is at the core of sexual addiction, be it pornography or partnered sex. Men show a stronger Coolidge effect than women (Hughes et al., 2021), which fits with the greater percentage of sexually-addicted men. Sexual novelty boosts dopaminergicneurotransmission at the nucleus accumbens (Fiorino et al., 1997).
11. A reply to some specific criticisms of the notion of sex addiction
Walton et al. (2017) write:
“…….the conceptualization of sexual behavior as an addiction has long been criticized, as research has failed to substantiate physiological conditions of tolerance and withdrawal.” Similarly, Prause et al., (2017, p.899) write.
“However, experimental studies do not support key elements of addiction such as escalation of use, difficulty regulating urges, negative effects, reward deficiency syndrome, withdrawal syndrome with cessation, tolerance, or enhanced late positive potentials.” and (p.899):
“Sex does not allow for supraphysiological stimulation.” Neves argues (p.6).
“….in sexual behaviours, the elements of risky use, tolerance and withdrawal are not present.”
As discussed next, the evidence does not support the arguments just referenced in this section.
11.1. Difficulty regulating urges
There is abundant evidence derived from discussions with patients of their severe difficulties in regulation (Gerevich et al., 2005). Some sexually-addicted people are even driven to consider suicide as the only way out (Garcia and Thibaut, 2010, Schneider, 1991).
11.2. Tolerance, risk and escalation
Tolerance, risk and escalation need to be considered together since logic suggests that they are manifestations of a common process. Neves (2021, p.6)describes the criterion of tolerance as.
”…. the person needs to do more of it to achieve the same effect”.
This applies to drugs, in increasing the dose over time, but Neves argues that it does not apply to sex. It is hard to compare doses of drug and sex. However, the corresponding increase in sex could be an increased time spent on the activity or increasing the deviation from conventional behavior (Zillmann and Bryant, 1986), e.g. the shock value as in looking at child pornography (Kasl, 1989, Park et al., 2016).
Some sexually-addicted people run high risks in pursuing sex (Bancroft et al., 2003, Garner et al., 2020, Kafka, 2010, Miner and Coleman, 2013), described as searching for “hits of adrenalin” (Schwartz and Brasted, 1985, p.103). The amount of time spent and the level of risk escalate over time (Carnes, 2001, Reid et al., 2012, Sunderwirth et al., 1996). Schneider (1991)observed a progression of sexual addiction characterized by trying new behavior and increasing risks in order to gain the same ‘high’. Hunter (1995)and Dwulit and Rzymski (2019) observed a progression to more extreme content of pornography over time. In one study, 39 out of 53 participants reported tolerance, in needing to spend time more often in their sexual activity to get the same effect (Wines, 1997).
In the phenomenon known as bug-chasing, gay men seek unprotected sex with men who are positive for the HIV virus (Moskowitz and Roloff, 2007a). The assumption is that they are seeking (p.353):
“.the uncertainty and the risk derived from unprotected sex.”
Moskowitz and Roloff (2007b) suggest that this fits a model of sexual addiction, with escalation to the “ultimate high”. There is a correlation between an individual’s score on the sexual compulsivity scale and the tendency to engage in high-risk sexual activities, such as sexual marathons (Grov et al., 2010).
11.3. Reward deficiency syndrome
The evidence for reward deficiency syndrome at the basis of addictive activities becomes steadily weaker. For example, it cannot explain pathological overeating, sometimes identified as feeding addiction, while the incentive motivation model can do so (Devoto et al., 2018, Stice and Yokum, 2016).
Leyton and Vezina (2014) appear to have solved the conundrum on whether too little or too much dopamine activity lies at the basis of motivation. Considering the behavior to which a person is addicted, there is hyperactivity in the dopamine pathway in response to the addictive cue. The reaction to cues to behavior for which the person is not addicted shows hypoactivation. Further evidence leading to the conclusion of hyperactivity of dopamine underlying addictive activity will be presented when Parkinson’s disease is discussed (Section 13.5).
11.4. Withdrawal symptoms
Similar to Prause et al. (2017), Neves (2021, p.7) argues that withdrawal symptoms from sexual activity do not exist. Walton et al. (2017) assert that the notion of sex addiction runs into trouble because of an absence of physiological signs of withdrawal.
Some sexually addicted patients report withdrawal symptoms, including on occasion similar to those of drug, even cocaine, addiction (Antonio et al., 2017, Chaney and Dew, 2003, Delmonico and Carnes, 1999, Garcia and Thibaut, 2010, Goodman, 2008, Griffiths, 2004, Paz et al., 2021, Schneider, 1991, Schneider, 1994). Symptoms include such things as tension, anxiety, irritability, depression, disorder of sleep and difficulty with work (Gerevich et al., 2005, Hunter, 1995, Kasl, 1989). Some of Carnes (2001) patients described agonizing withdrawal symptoms. In one sample of people reporting sex addiction, 52 out of 53 experienced withdrawal symptoms, such as depression, insomnia and fatigue, the latter two also being associated with withdrawal from stimulants (Wines, 1997).
Unless one believes in dualism, all psychological phenomena correspond to physiological changes (Goodman, 1998). The relevant distinction is surely between withdrawal symptoms that are observed in the body outside the brain (e.g. wet-dog shakes, goose bumps) and those which are not. By this criterion, alcohol and heroin would clearly qualify whereas cocaine, gambling and sex typically would not (Wise and Bozarth, 1987). But a pain based only in the brain/mind following cessation of use is surely no less painful.
11.5. Supraphysiological stimulation
The presence of drugs or food taken in excess of physiological needs represent events in the body outside the brain. However, so-called behavioral addictions are associated with supraphysiological stimulation and plasticity within regions of the brain that also show these effects in response to addictive drugs, (Olsen, 2011), (Section 3.4).
11.6. Enhanced late positive potentials
Steele et al. (2013) examined a population of men and women who reported having problems with on-line pornography. The stimuli were static images and the P300 potential was measured. The authors claimed that the P300 amplitude was a measure of sexual desire rather than sexual addiction.
There are several problems with this study (Love et al., 2015, Wilson, 2017). Seven participants did not identify as heterosexual, so they might not have been sexually aroused by the heterosexual imagery. Hilton (2014) pointed out the absence of any control group. The static images, including merely caressing, might have produced a much-reduced response compared to the moving images most likely to have been used normally by the participants (Wilson, 2017). Steele et al. note that most addicted people masturbate during viewing and here they were prevented from doing so, which again might have contributed to a contrast effect. A further consideration concerns what the changes in potential were actually reflecting: response to the image or anticipation of the image? As far as responses of the ventral striatum are concerned, only the anticipation phase distinguishes between problematic and non-problematic individuals. It could be that a similar principle applied here.
12. Binges
As with alcohol and feeding, people showing problematic sexuality sometimes binge, e.g. extensive masturbation accompanied by pornography (Carnes et al., 2005). Walton et al. (2017) describe an apparently similar phenomenon termed ‘sex benders’, i.e. multiple sexual encounters apparently in a dissociated state. Wordecha et al. write (2018, p.439).
“All patients declared that during pornographic binges they initially experienced positive emotions (e.g., excitement and pleasure). Then, during the binge, most of the subjects do not have any specific thoughts (“cut off from thinking”) and dissociate from their emotions”.
Sessions of sexual binging are sometimes followed by ‘sexual anorexia’ (Nelson, 2003).
13. Comorbidity
Certain other conditions can give important insights into sex addiction, either by showing features in common with it or by being addictive in combination with sex. This section looks at several of these.
13.1. Combined addictions
Some patients show problematic use of sex and drugs/ alcohol, either at different times or in combination (Black et al., 1997, Braun-Harvey and Vigorito, 2015, Kasl, 1989, Långström and Hanson, 2006, Raymond et al., 2003, Schneider, 1991, Schneider, 1994, Timms and Connors, 1992). Some use alcohol to relax, overcome inhibitions and give the courage to ‘act out’ (Kasl, 1989).
Stimulants, such as cocaine and methamphetamine (‘extraversion drugs’), enhance desire and their problematic use can lock into association with sexual addiction (Antonio et al., 2017, Guss, 2000, Moskowitz and Roloff, 2007a, Sunderwirth et al., 1996). They are associated with increased risk-taking and delay discounting (Berry et al., 2022, Skryabin et al., 2020, Volkow et al., 2007).
Reid et al., (2012, p.2876) noted that.
“….those meeting criteria for methamphetamine dependence, reported using drugs so that they could act out sexually.”
In one study, some 70% of people addicted to sex were also addicted to cocaine (Washton, 1989)). Use of ketamine is also common (Grov et al., 2010) and boosting dopamine release in the ventral striatum is one of its effects (Vollenweider, 2000). Gamma-hydroxybutyrate (GHB) boosts dopamine release at low doses but not at high doses (Sewell and Petrakis, 2011) and is known to exert an aphrodisiac effect (Bosch et al., 2017).
Engaging in the one addictive behavior can trigger relapse in the other, described by Schneider as “reciprocal relapse”. Some sexually addicted patients report that, when reducing sexual behavior, another addictive activity, such as gambling, taking drugs or over-eating, increases. In one study, albeit on a small sample of people with problematic sexual behavior, the most common other excessive activities were pyromania, gambling, kleptomania and shopping (Black et al., 1997).
Investigators describe different types of ‘high’ (Sunderwirth et al., 1996, Nakken, 1996). The high obtained from sex and gambling, as well as stimulants such as cocaine and amphetamine, is termed an ‘arousal high’. By contrast, a ‘satiation high’ is associated with heroin and overeating. Heroin is not an aphrodisiac drug.
13.2. Attention deficit hyperactivity disorder (ADHD)
Comorbidity between ADHD and hypersexuality occurs (Blankenship and Laaser, 2004, Korchia et al., 2022). Treating ADHD can ease comorbid sexual addiction. There is broad agreement that ADHD is characterized as abnormalities in reward processing. Blankenship and Laaser (2004) note some similarities between sexual addiction and ADHD: a tendency to be a survivor of early trauma, an intolerance of boredom, stimulus-seeking and a lure towards high-risk behavior. ADHD is also characterized by a failure to take consequences into consideration when acting, something shared with borderline personality disorder (Matthies and Philipsen, 2014) (Section 13.3).
All agree that disruption of dopamine neurotransmission is of central importance in ADHD (Van der Oord and Tripp, 2020). However, the complexity of what exactly is the abnormality lies beyond the scope of the present review.
13.3. Borderline personality disorder (BPD)
Borderline personality disorder (BPD) appears to increase the vulnerability towards sexual addiction (Jardin et al., 2017). There is often comorbidity between sexual addiction and BPD (Ballester-Arnal et al., 2020, Briken, 2020). BPD is often associated with difficulties with emotional regulation, a search for instant gratification, increased frequency of drug addiction (the preference being crack or a combination of cocaine and heroin), sensation-seeking and behavioral addictions (Bandelow et al., 2010). In some cases, there is reduced inhibition on sexual behavior, revealed as risky sexual behavior and a large number of partners.
Considering the biological bases of BPD, there are some hints as to possible common origins with SA. Evidence points to a deficiency of serotonin, while the partial efficacy of antipsychotic agents suggest hyperactivity of dopamine (Bandelow et al., 2010 Ripoll, 2011). Bandelow et al. (2010) marshal evidence that at base in BPD is dysregulation of an endogenous opioid system, e.g. insensitivity of receptors or low levels of secretion.
13.4. Bipolar disorder
In bipolar disorder, the manic and hypomanic phases can look something like SA (Black, 1998). There is some comorbidity between bipolar disorder and behavioral addictions, a stronger effect with gambling addiction than sex addiction (Di Nicola et al., 2010, Varo et al., 2019). The manic/hypomanic phase is associated with elevated dopamine levels (Berk et al., 2007).
13.5. Parkinson’s disease (PD)
A number of patients treated with dopamine agonists and L-Dopa show “pathological hypersexuality”, which is troubling to them or their families or both. This behavior is wholly out of character, e.g. paedophilic desire, exhibitionism or coerced sex. This suggests that a boost in dopamine levels triggers a search for sexual novelty (Klos et al., 2005, Nakum and Cavanna, 2016, Solla et al., 2015).
Some PD patients show problematic gambling, on its own or in association with problematic sexuality. Cessation of the medicine is followed by loss or at least amelioration of the excessive behavior. If the behavior were simply correcting negative affect, it is unclear why it should cease with the cessation of medication that targets dopamine.
Parkinson’s patients with hypersexuality and shown sexual images reveal an increased response in the ventral striatum when on their medication compared to the time off (Politis et al., 2013). They also reveal sensitization of the system (O’Sullivan, et al., 2011). These effects also occur in drug and sexual addiction (Section 3.4). As with addictions, there is a dissociation between wanting and liking: PD patients do not rate the erotic stimuli more strongly in terms of liking.
The fact that hypersexuality arises when dopamine levels are boosted is incompatible with the dopamine deficiency model. Rather, it favors an incentive motivation model, being based on elevations of dopamine (Berridge and Robinson, 2016).
13.6. Stress
Acute stress plays an important role in accentuating sexually-addictive behavior (Bancroft and Vukadinovic, 2004, Carnes, 2001, Kafka, 2010). Stress diminishes the inhibition exerted by the goal-based control (Bechara et al., 2019). At the same time, it increases the sensitivity of the excitatory dopaminergic pathway (Peciña et al., 2006). Thereby, it reduces the capacity to restrain behavior and increases the sensitivity to sexual cues.
13.7. Depression
Some sexually addicted men find their desire to be highest at times of depression (Bancroft and Vukadinovic, 2004). Evidence suggests that dopamine activity is low at such times (Shirayama and Chaki, 2006). This might seem to be incompatible with incentive motivation principles and to favor reward deficiency theory. However, it could be that the desire for all activities is reduced but that for sexual activity still comes out top (Perales et al., 2020). Another possibility, not incompatible with this, is that the men have a memory of past encounters which lifted their mood. This is rather as one might have a memory of taking aspirin for a headache.
14. Development
14.1. Timing
The tendency for an activity to become addictive depends upon when it was first performed, adolescence and early adulthood representing the most vulnerable period for both drug (Bickel et al., 2018) and sexual (Black et al., 1997, Hall, 2019, Kafka, 1997) addictions. Voon et al. (2014) found that a sample of young men who developed problematic pornography use first started viewing at an average age of 14 years, whereas controls with unproblematic viewing started at 17 years. A large percentage of sexually-addicted men started viewing pornography even before the age of 12 (Weiss, 2018).
14.2. Attachment theory
An assumption that permeates the literature is that addiction is usually the outcome of a failure of early infant attachment (Adams and Love, 2018, Beveridge, 2018, McPherson et al., 2013). That is to say, there is a failure to find secure attachment. This triggers the search for compensation, which might be drugs, or, as in the present case, sex. The solution that is discovered provides a source of self-soothing. How is the solution found? It could be, say, accidental touching of the genitals leading to masturbation or modelling of the sexual behavior of peers.
14.3. Brain development
The brain mechanisms of interest here show a distinctive pattern of development: subcortical regions involved in incentive motivation develop faster than the prefrontal regions that exert inhibition in the interests of long-term consequences (Gladwin et al., 2011, Wahlstrom et al., 2010). This results in adolescence being a time when there is maximum misalignment and hence dominance of the sub-cortical appetitive system (Steinberg, 2007). Engaging in activities at this stage increases the chances that they will become addictive. Most of the evidence derives from drug addiction but it seems reasonable to extrapolate to problematic sexuality. Abuse appears to increase the disparity and hence make addiction more likely.
14.4. The effects of early abuse
The chances of showing any of a number of addictive activities in adults, including drug use, sex and problematic eating are increased with childhood abuse (Carnes and Delmonico, 1996, Smith et al., 2014, Timms and Connors, 1992). There are pointers to a correlation between severity of childhood abuse (particularly sexual abuse) and the number of addictive activities (including problematic sexuality) when adult (Carnes and Delmonico, 1996; Cf. Långström and Hanson, 2006). Some sexually addicted people repeat the form of the sexual abuse that was inflicted on them as children, either repeating the role of victim but now voluntarily so or playing the abuser’s role (Firoozikhojastehfar et al., 2021, Kasl, 1989, Schwartz et al., 1995b).
14.5. Explaining the effects of abuse
Evolutionary considerations can give possible insight into how a tendency to addiction arises. Belsky et al. (1991) suggest that the developing child forms an unconscious assessment of its environment and the degree of stability that it offers. Where much uncertainty is involved, e.g. broken family, changing parental partners and/or frequent moves of home, the process of sexual maturation of the child is accelerated. The child then has the tendency to produce offspring with minimal investment of resources in any one of them. The evolutionary logic is that opportunities for mating are seized when available. Conversely, a stable family environment is associated with a child’s relatively late sexual maturation. Mating is delayed and is associated with high investment in any offspring.
Alley and Diamond (2021) describe early life adversity (ELA), which refers to physical, psychological or sexual abuse or any combination of these. Evidence is presented that individuals who suffered from ELA have a higher tendency to show risk-taking in their sexual behavior. This is manifest in such things as early sexual debut, early pregnancy, catching sexually transmitted diseases and a relatively high number of sexual partners.
What are the mechanisms by which ELA has this effect? Alley and Diamond review evidence concerning such things as peer influence and problematic parenting. They then ask how these factors mediate their role on sexual behavior in terms of the young person’s decision-making and answer: “heightened sensitivity to sexual reward”. Adversity early in life and at the time of puberty sets the balance between risk-taking and safety, giving an outcome biased towards immediate sexual pleasure and sensation seeking (a ‘fast strategy’) and away from delaying gratification.
As just noted, adolescence is generally the time of maximum risk-taking. However, Alley and Diamond (2021) review evidence that children and adults who suffered early adversity tend to show risk-taking more typical of adolescents.
15. Alternative explanatory models
Various terms exist to describe out-of-control sexuality. Some refer to a well-researched and well-established process or personality type. This section looks at four such: hypersexuality, obsessive-compulsive disorder, impulsive disorder and a high drive. In the literature, one finds two ways of discussing the relationship between these terms and sexual addiction:
- 1.
-
As alternative models that account better for the phenomena than does the label ‘addiction’.
- 2.
-
Processes that can co-exist with an addictive process.
This section will argue that the term ‘drive’ is outmoded. Hypersexuality, compulsivity and impulsivity can co-occur with problematic sexuality (Bőthe et al., 2019). However, it will be argued that, considering a population with problematic sexuality, they cannot be used as all-encompassing descriptions.
15.1. Too much sex or too high a desire: hypersexuality
Hypersexuality is defined in DSM-5 as “a stronger than usual urge to have sexual activity” (cited by Schaefer and Ahlers, 2018, p.22). Carvalho et al. (2015) distinguish between individuals with hypersexuality and those with problematic sexuality. Only the latter might constitute ‘addicted’, the former simply being described as having a passion (Perales et al., 2020).
The definition of ‘hypersexuality’ rather than ‘addictive’ would fit the sample of women studied by Blumberg (2003). They reported intense desires for sex, which they acted upon, with some social rejection of their behavior. However, they reported being happy with their situation and did not seek help to correct it. Blumberg rejected the label of ‘addicted’ to describe them. Indeed, a fundamental criterion of addiction is not one of the amount of sex but one of conflict, suffering and a wish to change.
15.2. Obsessive-compulsive disorder (OCD)
The word ‘compulsion’ captures a feature of the mental life of sexually-addicted people, i.e. a feeling compelled to act, often against their better judgement (Perales et al., 2020). So, can sexual addiction be classified as a form of OCD?
15.2.1. Coleman’s argument and the counter argument
In a very influential article, Coleman (1990) states (p.9):
“Compulsive sexual behavior is defined here as behavior that is driven by anxiety reduction mechanisms rather than by sexual desire”.
Coleman argues that patients with what he calls compulsive sexual behavior (CSB) (p.12):
“….rarely report pleasure in their obsessions or compulsive behavior”.
In reality, there are numerous reports of sexual arousal and pleasure, even extreme pleasure, from sexually addictive activities (e.g. Bostwick and Bucci, 2008; Delmonico and Carnes, 1999; Firoozikhojastehfar et al., 2021; Levi et al., 2020; Reid et al., 2015; Schwartz and Abramowitz, 2003).
Kowalewska et al., (2018, p.258) concluded.
“Together, these findings do not show strong support for considering CSB as an obsessive-compulsive-related disorder”.
The overlap between obsessive-compulsive disorder and out-of control sexual behavior is small (Bancroft, 2008, Kafka, 2010, Kingston and Firestone, 2008). Reid et al., (2015, p.3) claim that.
“…very few hypersexual patients also meet criteria for an obsessive compulsive disorder”.
15.2.2. Contrasting sexual addiction and OCD – behavior and conscious experience
There are further arguments against seeing sexual addiction as a form of obsessive-compulsive disorder (Goodman, 1998, Kafka, 2010). Sexual addiction is rooted in pleasure-seeking and positive reinforcement, with a possible shift to aversive-avoidance and negative reinforcement after repeated experience (Goodman, 1998). By contrast, OCD is rooted in negative reinforcement with a possible element of positive reinforcement if the act is felt as achieving completion.
People with OCD can also experience sexual themes in the content of their obsession but these have a very different affective quality from those of addicted individuals. Schwartz and Abraham (2005) write that sexually-addicted people (p.372):
“…experience their repetitive sexual thoughts as erotic and not particularly distressing. In contrast, patients with OCD report experiencing repetitive sexual thoughts as highly repugnant and irrational.”
The thoughts of the OCD patients were associated with very high fear and avoidance, whereas by contrast the sexually-addicted showed very low levels. The SA group reported deliberately acting upon their sexual thoughts to trigger the corresponding action, whereas the OCD group reported taking action to attempt to neutralize them and none engaged in the corresponding behavior. Exposure and response prevention are appropriate treatments for OCD but extreme caution is needed in SA so as not to sensitize the system (Perales et al., 2020). Carnes (2001, p.36) describes the experience of certain addicted people as “the excitement of the illicit”. Typically, the OCD individual is obsessed by perfectly legal things such as checking and washing. Sensation-seeking characterizes out-of-control sexual behavior, whereas anxiety avoidance is a hallmark of OCD (Kingston and Firestone, 2008).
In principle, an addicted individual and an OCD sufferer could experience the same repetitive intrusive thought, e.g. an image of having sex with a child. The addicted individual might be sexually aroused by the thought, seek pornography that depicts it to accompany masturbation and be moved to consider realizing the imagery in reality. By contrast, the OCD sufferer would typically be horrified by the thought, seek evidence to prove that he had never done such a thing, pray for strength to resist and take steps to avoid being near children. Sexual imagery of the OCD sufferer is very rarely put into action (Kingston and Firestone, 2008). All this is very different from addictive sexual behavior, where the goal is usually to put the imagery into action. The fact that anti-androgen medications are sometimes successful in treating sexual addiction (Schwartz and Brasted, 1985) points against obsessive-compulsive disorder being the explanation.
15.2.3. Tantalizing experiences
There are caveats to the argument that addictive thoughts are purely positive. One of these is discussed in connection with addiction to drugs (Kavanagh et al., 2005), extrapolated to non-drug addictions (May et al., 2015). They argue that intrusive thoughts on the addictive activity can be tormenting if there is little chance of realizing them in action. Of course, the comparable OCD sufferer fears precisely realizing them.
An addicted individual might resist the thoughts, not because they are intrinsically aversive but to reduce the chances of discovery (Goodman, 1998). On starting therapy for sexual addiction, most clients in one study were ambivalent about wanting to change (Reid, 2007). It is highly unlikely that OCD patients would feel the same way, though they might well feel fear and ambivalence at the prospect of, say, exposure therapy. Preventing the response typically triggers anxiety in an OCD sufferer but rage in an addicted individual (Goodman, 1998).
15.3. An impulse control disorder
An aspect of impulsivity can be defined as favoring immediate rewards over long-term rewards (Grant and Chamberlain, 2014). By this criterion sexually-addicted people do show impulsivity. For out-of-control sexuality, Barth and Kinder (1987) suggest that we use the term ‘atypical impulse control disorder’. However, only around 50% of patients seeking help for problematic sexuality show evidence of the generalized impulsivity that would suggest inadequate general top-down controls (Mulhauser et al., 2014).
The literature describes two types of impulsivity: domain-general, which is evident regardless of the task, and domain-specific, where the level of impulsivity depends upon the context (Perales et al., 2020, Mahoney and Lawyer, 2018). Mulhauser et al. raise the possibility that, in problematic sexuality, impulsivity might only be shown in the presence of sexual cues.
Sexually-addicted people often display a lengthy planning phase, e.g. scanning internet sites for promising contacts, exploiting full conscious cognitive resources (Hall, 2019), i.e. the process of Box C (Table 1). They also show an amazing ability to lie and deceive about their intentions and actions, e.g. to their spouses (Carnes, 2001). Successful lying requires quite the opposite processing to that underlying impulsivity, i.e. the performance of goal-directed behavior aided by inhibition of the expression of the truth. This suggests that, although there can be an aspect of impulsivity in this behavior, sexual addiction should not be treated simply as an impulse-control disorder.
15.4. Other forms of psychological disturbance
15.4.1. Comorbidity
Some critics argue that so-called sexually-addicted people are really manifesting some underlying problem such as PTSD, alienation, depression or anxiety, for which sexual behavior is merely self-medication. Some sexually addicted people note a mood of depression or sadness experienced at the time of engaging in their addiction (Black et al., 1997). The co-morbidity between (i) sexual addiction and (ii) anxiety and mood disorders is high, estimates being up to 66% (Black et al., 1997) or even 96% (Lew-Starowicz et al., 2020). Ley (2012, p.79) asserts that:
“One hundred percent of the people who seek sex addiction treatment have some other major mental illness, including alcohol and drug addictions, mood disorders, and personality disorders.”
Ley gives no reference to this claim, which seems dubious but even if it were true, it does not cover those who do not seek treatment. Co-morbidity with psychological distress is equally true of any addiction whether it is to drugs or gambling or whatever (Alexander, 2008, Maté, 2018). But, of course, this does not mean that such things as drug addiction do not exist as distinct entities.
Expressed in alternative terms, a failure of emotion regulation is of central importance to all recognized addictions. Insecure attachment is often a feature of addictions (Starowicz et al., 2020) and this points to the validity of describing out-of-control sexual behavior in terms of addiction.
15.4.2. The sequence of comorbidity
Although the co-morbidity with forms of psychological distress is high, there is a fraction of people showing out-of-control sexual behavior for whom there is no evidence of any prior problem (Adams and Love, 2018, Black et al., 1997, Hall, 2019, Riemersma and Sytsma, 2013). Distress can be caused by the addiction rather than being a cause of it. Only some with problematic sexuality report that their urges are highest at times of depression/anxiety (Bancroft and Vukadinovic, 2004). Quadland (1985) found that his group of men showing problematic sexuality had no more “neurotic symptoms” than the control group. Some report that their sexual activity corresponds to a positive mood (Black et al., 1997).
15.5. A high drive
Rather than ‘sex addiction’, some argue that it would be better to use the term ‘high sex drive’. However, as Kürbitz and Briken (2021) argue, ‘high drive’ should not be used to describe sexual addiction since ‘high drive’ does not imply suffering. The term ‘drive’ largely went out of use in motivation research several decades ago, even though it appears sometimes in the literature on problematic sexuality (Braun-Harvey and Vigorito, 2015, Hunter, 1995). Walton et al. (2017) refer to a ‘biological drive’. If drive means anything at all (as in its use by Freud, 1955 and Lorenz, 1950), then it implies that behavior is pushed from within by some accumulating uncomfortable pressure that needs discharge (the pressure-cooker analogy).
Sexually addicted people do not exhibit an unfocussed push towards any sexual outlet. Rather they can be highly selective in what they pursue (Goodman, 1998, Kafka, 2010, Schwartz and Brasted, 1985). Schwartz et al. (1995a) note the existence of the phenomenon of (p.11).
“Having chronic affairs with strangers, combined with sexual inhibitions with one’s own husband or wife”.
Others ignore a sexually willing and objectively attractive partner to watch porn movies or masturbate to fantasy about women (Black, 1998) or are only turned on by using sex workers (Rosenberg et al., 2014). For his sample of gay and bisexual males, Quadland (1985) discovered that those showing compulsive sexual behavior desired a much lower number of partners than they actually had. However, without therapy they were unable to achieve this number. He saw this as evidence against their having a “higher sex drive”. In other words, their ‘wanting’ was at odds with their wanting (Table 1).
All this sounds much more like incentive capture by supernormal stimuli rather than the urgency provoked by an uncomfortable general drive. In other words, incentive motivation theory marries well to sex addiction and the pursuit of one or more particular incentives.
The arousal of motivation by incentives, rather than there being any abnormal elevation of a general drive, can accommodate the idiosyncratic nature of some forms of sexual addiction. For example, some sexually-addicted men reveal a fetishist element in their arousal (Black et al., 1997, Kafka, 2010), e.g. cross-dressing or viewing pornography showing women urinating (Carnes, 2001) or are into inherently risky activities such as unsafe sex, exhibitionism or voyeurism (Schwartz and Brasted, 1985).
16. Sexual offending
16.1. Basics
Without citing evidence, Ley (2012, p.140) claims that.
“First, for most sexual offending, sexuality plays only a small part in the act”.
This assumption once advanced by feminists has repeatedly been refuted (Kasl, 1989, Palmer, 1988), a modern interpretation being that a combinationof desire for sex and domination is at the motivational basis of sexual offending (Ellis, 1991). Sex offenders tend commonly to show poor attachments, something associated with addiction (Smith, 2018b). However, not all sexual offenders show such background predisposing factors. For example, those watching child pornography can start with legal pornography and progress to illegal, getting captured by the potency of the imagery (Smith, 2018b).
Carnes (2001), Herman (1988), Smith (2018b) and Toates et al. (2017) argue that some sexual offending can be better understood with a sex addiction model. As with other addictions, habitual sex offenders usually start offending in adolescence. Escalation commonly occurs from less to more serious types of offending (Carnes, 2001). Paedophiles who prefer boy victims show a strong tendency to have been abused as children, suggesting a kind of imprinting process (Beard et al., 2013). The offense might be planned a long-time before its execution, which argues against offending simply being the result of a failure of impulse-control (Goodman, 1998).
The sentence of Harvey Weinstein to prison triggered much speculation about the existence or otherwise of sex addiction and its relevance to his case. Weinstein attended an expensive clinic dedicated to treating sex addiction and this action has been a favourite target for the cynicism of those who dismiss the notion of sex addiction.
Whether sex addiction exists is one question. Whether Weinstein ticks the boxes of addiction is a quite different question and the two should not be conflated. Why, at least in principle, can’t someone be both a sex addict and an offender? These are two quite distinct orthogonal dimensions.
16.2. Fantasy and behavior
In people with problematic sexuality and where the fantasy is sexually arousing and hedonically positive, there is a tendency to enact in behavior the content of the fantasy (Rossegger et al., 2021). Both men and women entertain coercive fantasies but men more frequently than women (Engel et al., 2019). Not surprisingly, men are much more likely to enact the violent fantasy in reality.
16.3. Lust killing
Some features of sexual serial killing suggest an underlying addiction. Borderline personality disorder is strongly represented amongst such killers (Chan and Heide, 2009). Some killers report ambivalence in their behavior, while escalation from relatively less serious behavior (e.g. voyeurism, exhibitionism), through rape, to serial lust killing is common amongst them (Toates and Coschug-Toates, 2022).
A number of lust killers report personal insights that are compatible with addiction. Arthur Shawcross described the transition from aversion to killing to attraction (Fezzani, 2015). Michael Ross reported being assailed by appetitive images and their intensity being reduced by anti-androgen treatment, something he published in the journal Sexual Addiction and Compulsivity (Ross, 1997).
17. Cultural factors
Some critics suggest that sex addiction represents a social construction. For example, Irvine (1995) considers it to be a “social artifact” and writes:
“…the sex addict is a historical character constructed from the sexual ambivalences of a particular era.”
It would be hard to imagine two cultures more different than 1980 s USA and Iran today and yet sexual addiction is clearly evident in both cultures (Firoozikhojastehfar et al., 2021). Irvine continues by questioning (p.431):
“…the very concept of sexual addiction – that there can be too much sex…”.
This might represent the position of some who employ the notion of sex addiction but is not the position of its best-known advocates. Thus, Carnes and colleagues write (Rosenberg et al., 2014, p.77):
“Caution in diagnosing sex addiction or related disorders is justified. The majority of those who have multiple affairs, who are promiscuous, or who take part in novel expressions of sexuality are not sexually addicted”.
Irvine writes (p.439);.
“When deviance is medicalized, however, its origins are located within the individual.”
She criticizes believers’ (p.439):
“….emphasis on the brain as the site of sexual impulses”.
An incentive motivation model can answer this. Desire arises from a dynamic interaction between the brain and its external environment. There is no dichotomy to be drawn.
Levine and Troiden (1988, p.354) state:
“In the permissive climate of the 1970 s, it had been unthinkable to argue that there were people who were “addicted to sex”…”.
Unthinkable or not, it was in 1978 that Orford published his classic text identifying the problems of out-of-control sexuality (Orford, 1978).
18. Erectile dysfunction
The link between pornography viewing and erectile difficulties presents what might appear to be a confusing picture. Prause and Pfaus (2015) found that longer hours of watching pornography were not associated with erectile difficulties. However, their participants were described as “non-treatment seeking men” so it cannot be concluded that even the high end met criteria of addiction. Other articles downplay the seriousness and extent of the phenomenon (Landripet and Štulhofer, 2015) though it is unclear whether the samples on which such conclusions are based met the criteria of addiction.
Other evidence suggests that erectile dysfunction can be a consequence of sexually-addictive activity (Jacobs et al., 2021). Park et al. (2016) review a number of studies showing this effect: erectile capacity maintained in the context of watching pornography, while erectile dysfunction is shown in the context of a real partner (Voon et al., 2014). Raymond et al. (2003) give a lifetime percentage of 23% of their sample exhibiting this.
Park et al. (2016) suggest that a contrast effect is involved: the reaction of the dopamine system is inhibited by the failure of the real woman to match the endless novelty and availability of the on-line pornographic images. A study on homosexual males also points in this direction (Janssen and Bancroft, 2007). These males showed erectile difficulties on viewing vanilla pornography, as contrasted with the more extreme pornography that they had earlier viewed.
19. Relevance to treating sexual addiction
19.1. A guiding philosophy
As a general principle, it appears that the sexually-addicted individual has an excess weight of excitation relative to inhibition (Briken, 2020). Therapeutic techniques implicitly involve increasing the relative weight of inhibition. A book entitled Treating Out of Control Sexual Behavior: Rethinking Sex Addictiondisapproves of the sex addiction label (Braun-Harvey and Vigorito, 2015). Somewhat ironically, the authors describe with approval the notion of competition in the brain between different types of control that has been so successfully applied to drug addiction (Bechara et al., 2019). Braun-Harvey & Vigorito describe the powerful role of (i) novelty and conversely habituation and (ii) proximity to the object in space and time, all cardinal features of incentive motivation. In effect, their favored therapy involves trying to recalibrate the relative weight of stimulus-based and goal-based in favor of the latter.
19.2. Biological interventions
The fact that selective serotonin reuptake inhibitors are sometimes effective as a treatment for problematic sexuality, does not enable a distinction to be made with OCD since they are also prescribed for this. However, they are thought to underlie inhibition and so presumably their efficacy is exerted there (Briken, 2020).
The success of the opioid antagonist naltrexone in treating sex addiction, also used to treat drug addiction, (Grant and Kim, 2001, Kraus et al., 2015, Sultana and Din, 2022) is compatible with an addiction model for sexual behavior. The successful use of testosterone blockers in the most serious cases (Briken, 2020) also points to the addictive nature of out-of-control sexuality.
In addition to the use of drugs, non-invasive excitatory electrical stimulation of the prefrontal cortex, having as target the dorsolateral prefrontal cortex, might be employed, as in treating drug addiction (Bechara et al., 2019).
19.3. Psychotherapeutic techniques
As a broad generalization, a number of psychotherapeutic interventions involve goal-setting (e.g. achieving non-addictive sexuality) and thereby inhibition upon behavioral tendencies that are at odds with the high-level goal of correcting the addictive condition. The technique of episodic future thinking attempts to strengthen the power of cognitions related to the future and has been used in treating drug addiction (Bechara et al., 2019).
Using acceptance and commitment therapy (ACT), Crosby and Twohig (2016)treated patients for pornography addiction by amongst other things increasing the frequency of (p.360) “high quality of life activities.” Mentalization-based therapy involves “intentionality and volition”, with a primary goal of “cultivating a sense of agency and personal control (Berry and Lam, 2018). Berry and Lam (2018, p.231) note that.
“.many patients use sexually addictive behaviours to help them cope with difficult feelings but are unaware of this function.”
19.4. Behavioral interventions
Alternatives to the addictive activity could be encouraged and reinforced (Perales et al., 2020). To resist temptation, patients can be encouraged to carry a picture of a loved one, to be inspected at times of temptation (Smith, 2018b). This could be interpreted as bringing an otherwise remote consideration into the present and control of behavior into alignment with non-addictive goals.
When in a cold state it can be very difficult to predict behavior that would arise in a hot state. Therefore plans can be established in a cold state, such as ‘avoid being near schools and swimming pools’ in the hope that the patient does not get into a hot state. Hall (2019, p.54) refers to “seemingly unimportant decisions”. She exemplifies this with a man who ‘just happened to be in Soho2’ and when there gave into temptation. However, he had planned his business meeting to be in London and withdrawn money from the bank weeks prior to this. It is at the relatively cool stage of planning when behavioral interventions might be most successful. Just one look at Soho for old-time’s sake might prove catastrophic.
19.5. Some possibly useful reflections
Vigorito and Braun-Harvey (2018) suggest that a person might sincerely love a partner but still give in to temptation. The lapse should not be thought to invalidate the conscious goal of trying to maintain fidelity. They write (p.422):
“……framing out of control behavior within the dual process model conceptualizes contradictory behaviour as quintessentially human, seen in the same imperfect and dynamic process that describes much of human behaviour and its problems.”
Hall (2013) describes a patient who reported to his wife that he used sex workers and pornography but no longer enjoyed either. The wife asked the therapist whether such a distinction is possible and was told that it is. She replied that she could forgive him given that he no longer enjoyed these things.
20. Conclusions
There might never be a definition of sexual addiction or even addiction in general to which everyone subscribes. So, a dose of pragmatism is needed of the kind – does out-of-control sexual behavior exhibit a number of features in common with the classical addiction shown towards hard drugs? By this criterion, the evidence gathered here points strongly to the validity of the label of ‘sex addiction’.
To assess whether the notion of sex addiction is valid, the present paper points to a number of criteria:
-
1. Is there evidence of suffering for the individual and/or any family members?
-
2. Does the individual seek help?
-
3. Is wanting out of proportion to liking, when compared with the situation prior to showing problematic sexuality or compared to controls?
-
4. Is the reactivity of the dopaminergic wanting pathway high in the context of sexual incentives by comparison with other incentives with which the individual does not have problems, such as food?
-
5. Does the individual feel withdrawal symptoms on ceasing the activity?
-
6. Is there escalation?
-
7. Does a shift towards increased weight of automaticity involving the dorsal striatum occur?
-
Does sex squeeze out most other activities such that life is suboptimal? This is the definition of drug addiction used by Robinson and Berridge (1993) and could equally be applied here.
If the answer to each question is ‘yes’, one might feel totally confident to argue for sexual addiction. A positive answer to question 4 might seem to be necessary for asserting its presence. One might claim that, if, say, 5/8 questions yield positive answers, then this is a strong pointer to sexual addiction.
On considering these criteria, the issue arises of whether a clear distinction between showing or not showing sexual addiction can be drawn. This problem equally arises in the context of other addictions, e.g. to drugs. In terms of the incentive motivation model, sexual addiction is based upon adjusting the parameters that are involved in conventional sexual behavior. That is to say, it does not involve any entirely new process to be added to the basic model, which suggests a continuum between no addiction and full addiction.
A slightly different criterion of addiction might suggest itself on identifying a process of positive feedback between increases in incentive sensitivity and increases in addictive behavior, a vicious circle. This could give a point of discontinuity, a lift-off of addictive activity. Similarly, decreases in inhibition with increases in addictive activity could also yield this effect. It is perhaps best left now to the reader to ponder these criteria!.
A number of features in common with drug addiction were highlighted and the biological bases of all such addictions is rooted in interactions between (i) dopaminergic and opioidergic neurotransmission and (ii) stimulus-based and goal-based processes. The evidence for a shift of weight of control from goal-based to stimulus-based, as a criterion of addiction (Perales et al., 2020) was presented as a weakening of liking relative to wanting.
The fact that people commonly show more than one addiction either simultaneously or in sequence suggests an underlying ‘addictive process’ (Goodman, 1998). This condition of disturbance appears to be that of affective state corresponding to dysregulated endogenous opioid activity. Opioid activity is associated with both positive and negative reinforcement.
The sexually-addicted individual appears to have discovered the reinforcing power of arousal-producing stimuli, as mediated by dopaminergic activity in the VTA-N.Acc. pathway. This is suggested by the tendency to develop addiction to risky activities and co-addictions to stimulant drugs.
The essential features of sex addiction can be illuminated by comparison with the phenomenon of food addiction and obesity. In its evolutionary origins feeding serves to keep nutrient levels within bounds. This is maintained by a system of (i) dopamine-based incentive motivation and (ii) reward based upon opioids. This worked well in our early evolution. However, given an abundance of processed foods, the system is overwhelmed and intake is far in excess of optimal (Stice and Yokum, 2016).
By analogy, addictive sex can be in response to, say, anxiety/stress and serves as self-medication. However, the potency of contemporary sexual incentives means that no such regulatory disturbance need be present for addiction to arise. Such considerations suggest that there need not be a dichotomy between regulation and non-regulation. Rather, there could be a continuum between good regulation and extreme lack of regulation (CF. Perales et al., 2020).
The characteristics of what constitutes sex addiction described here are probably the best that we can do. However, this analysis is not without its problems. As Rinehart and McCabe (1997) point out, even someone with a very low frequency of sexual activity might find this problematic and something to be resisted. Briken (2020) suggests that we do not describe as ‘addiction’ a situation of moral disapproval where the sexual behavior is of low intensity. Indeed, this would be disqualified by its not meeting the criterion of a shift towards stimulus-based control (Perales et al., 2020). Conversely, a person with a very high frequency might wreak havoc to family and colleagues but see no problem and hence would not qualify in terms of suffering to the self but would do so by that of a shift to stimulus-based control.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgments
I am very grateful to Olga Coschug-Toates, Kent Berridge, Chris Biggs, Marnia Robinson and the anonymous referees for various forms of support during this project.
Data availability
No data was used for the research described in the article.