The following is YBOP’s response to David Ley’s Psychology Today blog post “We Must Rely on Good Science in Porn Debate (2016).” Ley’s post is his response to Philip Zimbardo’s Psychology Today blog post “Is Porn Good For Us or Bad For Us?” (2016).
While Ley’s title says we must rely on “good science,” it is Ley who links to only a single paper (which actually supports the concept of porn addiction). In contrast, Zimbardo provides 14 references (13 studies, one article) and a link to his new book “Man, Interrupted: Why Young Men are Struggling & What We Can Do About It”. Zimbardo could have cited many more studies, as you will see.
David Ley Links to Only a Single Citation, and It Supports Porn Addiction
Ley provides plenty of bluster, but there’s not a single citation in Ley’s post that refutes anything in Zimbardo’s post. In fact, Ley’s article links to only one citation – which is a recent review of the literature on compulsive sexual behaviors, by Shane Kraus, Valerie Voon & Marc Potenza. Contrary to Ley’s claim, the “Voon review” actually supports the existence of porn addiction. An excerpt from the review:
“Overlapping features exist between CSB [compulsive sexual behavior] and substance use disorders. Common neurotransmitter systems may contribute to CSB and substance use disorders, and recent neuroimaging studies highlight similarities relating to craving and attentional biases.”
In other words, the research on CSBs has much in common with substance abuse disorders, even if cautious scientists want to see further evidence. Two of the authors of this review (Valerie Voon & Marc Potenza) are top addiction neuroscientists. Together they have published three studies on “porn addicts.” Two of the studies were fMRIs (brain scans), while one was neuropsychological (attentional bias). While Voon and Potenza tend to be very guarded, they stated that their three brain studies align perfectly with the addiction model (1, 2, 3). Ley ignores all of this and excerpts the cautious portion of the paper, which is a normal feature of serious scientific papers. Then he interprets it for us, claiming it means the data is conflicted (rather than merely still limited):
“Insufficient data are available regarding what clusters of symptoms may best constitute CSB (Compulsive Sexual Behavior) or what threshold may be most appropriate for defining CSB. Such insufficient data complicate classification, prevention and treatment efforts. While neuroimaging data suggest similarities between substance addictions and CSB, data are limited by small sample sizes, solely male heterosexual samples, and cross-sectional design.”
Read the above carefully. Yes, the researchers want more data. (They always do.) However, Kraus, Voon and Potenza clearly state that the existing data points for substance addictions and CSBs are neurobiologically similar. Simply put, drug addictions and compulsive sexual behaviors share similar neurobiological features and brain changes. By the way, nearly all the brain studies cited in this review to demonstrate that CSBs are very similar to substance abuse disorders involved compulsive internet porn users. It’s not surprising as a separate review (Neurobiology of Compulsive Sexual Behavior: Emerging Science. 2016) published a month earlier by Kraus, Voon and Potenza concluded:
“Given some similarities between CSB and drug addictions, interventions effective for addictions may hold promise for CSB, thus providing insight into future research directions to investigate this possibility directly.”
In other words, the conflict does not lie in the neuroscience on porn addicts, which is clear, and very similar to that on substance abusers. Instead, the conflict surrounds what “cluster of symptoms” best defines compulsive sexual behaviors (CSB). The difficulty agreeing on a cluster of symptoms arises from the fact that the researchers fail to tease apart sex addiction from Internet porn addiction, lumping them together as “CSBs.”
Update: Valerie Voon and other addiction researchers teamed up to write this commentary on the inclusion of the diagnosis of “compulsive sexual behaviour disorder” in the upcoming ICD-11: Is excessive sexual behaviour an addictive disorder? (Potenza et al., 2017) – You can see from the Excerpts that Valerie Voon fully supports the addiction model:
Compulsive sexual behaviour disorder (operationalised as hypersexual disorder) was considered for inclusion in DSM-5 but ultimately excluded, despite the generation of formal criteria and field trial testing. This exclusion has hindered prevention, research, and treatment efforts, and left clinicians without a formal diagnosis for compulsive sexual behaviour disorder.
Research into the neurobiology of compulsive sexual behaviour disorder has generated findings relating to attentional biases, incentive salience attributions, and brain-based cue reactivity that suggest substantial similarities with addictions. Compulsive sexual behaviour disorder is being proposed as an impulse-control disorder in ICD-11, consistent with a proposed view that craving, continued engagement despite adverse consequences, compulsive engagement, and diminished control represent core features of impulse-control disorders. This view might have been appropriate for some DSM-IV impulse-control disorders, specifically pathological gambling. However, these elements have long been considered central to addictions, and in the transition from DSM-IV to DSM-5, the category of Impulse Control Disorders Not Elsewhere Classified was restructured, with pathological gambling renamed and reclassified as an addictive disorder. At present, the ICD-11 beta draft site lists the impulse-control disorders, and includes compulsive sexual behaviour disorder, pyromania, kleptomania, and intermittent explosive disorder.
Compulsive sexual behaviour disorder seems to fit well with non-substance addictive disorders proposed for ICD-11, consistent with the narrower term of sex addiction currently proposed for compulsive sexual behaviour disorder on the ICD-11 draft website. We believe that classification of compulsive sexual behaviour disorder as an addictive disorder is consistent with recent data and might benefit clinicians, researchers, and individuals suffering from and personally affected by this disorder.
All 50 Neuroscience-Based Studies on Porn Users Support Zimbardo’s Claim; None support Ley’s
There’s a reason that Ley provided zero studies while Zimbardo tucked in 13. Truth be told, in 2016 Zimabardo could have cited 30 more neuroscience-based studies on CSB subjects. Put simply, Ley’s post omitted all 50 neuroscience-based studies on porn users that have been published in the last few years (up-to-date list). So far, the results of every “brain study” (MRI, fMRI, EEG, neuropsychological, neuro-endocrine) offer support for the concept of porn addiction. In addition to reporting the same fundamental brain changes as seen in substance addicts, a few studies also reported that greater porn use is associated with erectile dysfunction, decreased libido, anorgasmia, delayed ejaculation, and reduced neural response to images of vanilla porn.
The 41 studies on porn users also align with over 370 internet addiction “brain studies” (PET, MRI, fMRI, EEG) published in the last few years. Without exception, these studies report the same addiction-related brain changes as seen in substance addicts. Internet porn addiction is, according to various experts, a subtype of internet addiction as well as a CSB, as this recent review of the neuroscience literature pointed out: “Neuroscience of Internet Pornography Addiction: A Review and Update (2015).” Also see Sex Addiction as a Disease: Evidence for Assessment, Diagnosis, and Response to Critics (2015), which provides a chart that takes on specific criticisms and offers citations that counter them.
Finally, the real experts’ opinions on porn/sex addiction: this list contains 25 recent literature reviews & commentaries by some of the top neuroscientists in the world. All support the addiction model.
Addressing Specific Claims in David Ley’s Blog Post
DAVID LEY: “Dr. Zimbardo goes on to cite several studies and articles which have alleged that pornography has a neurological effect. Unfortunately, there’s the problem of causation versus correlation, again, something I learned about in basic research classes.”
RESPONSE: This single sentence demonstrates a profound lack of knowledge as to how research works.
When someone uses “no causation has been demonstrated” it makes listening scientists doubt that person’s basic understanding of science or research. When it comes to psychological and medical studies little research reveals causation directly. For example, all studies on the relationship between lung cancer and cigarette smoking are correlative – but cause and effect are settled.
In light of ethical requirements researchers are usually precluded from constructing experimental research designs which would prove pornography causes certain harms. Therefore, they must instead use correlational models. Over time, when a significant body of correlational studies are amassed in any given research area, there comes a point where the body of evidence can be said to prove a point of theory, even though there were no experimental studies. Put another way, no single correlation study could ever provide a “smoking gun” in an area of study, but the converging evidence of multiple correlational studies is used to establish evidence. When it comes to porn use, nearly every study published is correlative. To “prove” porn use is causing erectile dysfunction or addiction-related brain changes you would have to do one of two things:
- Have two large groups of identical twins separated at birth. Make sure one group never watches porn. Make sure that every individual in the other group watches the exact same type of porn, for exact same hours, and the exact same age. Continue the experiment for 30 years or so, followed by assessment of the differences.
- Eliminate the variable whose effects you wish to measure. Specifically, have porn users stop, and assess the changes months (years?) later. This is exactly what is occurring informally online as thousands of young men stop internet porn use to alleviate chronic non-organic sexual dysfunctions (that turn out to have been caused by porn use).
To this date only 10 studies have removed porn and observed the results. All 10 found significant changes. Seven of those studies had compulsive porn users with severe sexual dysfunctions abstain from porn. Those 7 studies demonstrate causation as patients healed chronic sexual dysfunctions by removing a single variable: porn. The 10 studies:
1) Trading Later Rewards for Current Pleasure: Pornography Consumption and Delay Discounting (2015) – This study reported that greater porn use was correlated with less ability to delay gratification. The researchers assessed porn users a month later and found that continued porn use correlated with less ability to delay gratification. Finally, researchers divided subjects into 2 groups: Half tried to abstain from their favorite food; half tried to abstain from internet porn. The subjects who tried to abstain from porn experienced significant changes: they scored better on their ability to delay gratification. The researchers said:
“The finding suggests that Internet pornography is a sexual reward that contributes to delay discounting differently than other natural rewards. It is therefore important to treat pornography as a unique stimulus in reward, impulsivity, and addiction studies and to apply this accordingly in individual as well as relational treatment.”
2) A Love That Doesn’t Last: Pornography Consumption and Weakened Commitment to One’s Romantic Partner (2012) – The study had subjects try to abstain from porn use for 3 weeks. Upon comparing the two groups, those who continued using pornography reported lower levels of commitment than those who tried to abstain.
3) Unusual masturbatory practice as an etiological factor in the diagnosis and treatment of sexual dysfunction in young men (2014) – One of the 4 case studies in this article reports on a man with porn-induced sexual problems (low libido, fetishes, anorgasmia). The sexual intervention called for a 6-week abstinence from porn and masturbation. After 8 months the man reported increased sexual desire, successful sex and orgasm, and enjoying “good sexual practices. Excerpts from the paper:
“When asked about masturbatory practices, he reported that in the past he had been masturbating vigorously and rapidly while watching pornography since adolescence. The pornography originally consisted mainly of zoophilia, and bondage, domination, sadism, and masochism, but he eventually got habituated to these materials and needed more hardcore pornography scenes, including transgender sex, orgies, and violent sex. He used to buy illegal pornographic movies on violent sex acts and rape and visualized those scenes in his imagination to function sexually with women. He gradually lost his desire and his ability to fantasize and decreased his masturbation frequency.”
In conjunction with weekly sessions with a sex therapist, the patient was instructed to avoid any exposure to sexually explicit material, including videos, newspapers, books, and internet pornography.
After 8 months, the patient reported experiencing successful orgasm and ejaculation. He renewed his relationship with that woman, and they gradually succeeded in enjoying good sexual practices.
4) Is Internet Pornography Causing Sexual Dysfunctions? A Review with Clinical Reports (2016) – An extensive review of the literature related to porn-induced sexual problems. Involving US Navy doctors, the review provides the latest data revealing a tremendous rise in youthful sexual problems. It also reviews the neurological studies related to porn addiction and sexual conditioning via Internet porn. The doctors provide 3 clinical reports of men who developed porn-induced sexual dysfunctions. Two of the three men healed their sexual dysfunctions by eliminating porn use. The third man experienced little improvement as he was unable to abstain from porn use.
Traditional factors that once explained men’s sexual difficulties appear insufficient to account for the sharp rise in erectile dysfunction, delayed ejaculation, decreased sexual satisfaction, and diminished libido during partnered sex in men under 40. This review (1) considers data from multiple domains, e.g., clinical, biological (addiction/urology), psychological (sexual conditioning), sociological; and (2) presents a series of clinical reports, all with the aim of proposing a possible direction for future research of this phenomenon. Alterations to the brain’s motivational system are explored as a possible etiology underlying pornography-related sexual dysfunctions. This review also considers evidence that Internet pornography’s unique properties (limitless novelty, potential for easy escalation to more extreme material, video format, etc.) may be potent enough to condition sexual arousal to aspects of Internet pornography use that do not readily transition to real-life partners, such that sex with desired partners may not register as meeting expectations and arousal declines. Clinical reports suggest that terminating Internet pornography use is sometimes sufficient to reverse negative effects, underscoring the need for extensive investigation using methodologies that have subjects remove the variable of Internet pornography use.
5) Male masturbation habits and sexual dysfunctions (2016) – It’s by a French psychiatrist who is the current president of the European Federation of Sexology. While the abstract shifts back and forth between Internet pornography use and masturbation, it’s clear that he’s mostly referring to porn-induced sexual dysfunctions (erectile dysfunction and anorgasmia). The paper revolves around his clinical experience with 35 men who developed erectile dysfunction and/or anorgasmia, and his therapeutic approaches to help them. The author states that most of his patients used porn, with several being addicted to porn. The abstract points to internet porn as the primary cause of the problems (keep in mind that masturbation does not cause chronic ED, and it is never given as a cause of ED). Excerpts:
Intro: Harmless and even helpful in his usual form widely practiced, masturbation in its excessive and pre-eminent form, generally associated today to pornographic addiction, is too often overlooked in the clinical assessment of sexual dysfunction it can induce.
Results: Initial results for these patients, after treatment to “unlearn” their masturbatory habits and their often associated addiction to pornography, are encouraging and promising. A reduction in symptoms was obtained in 19 patients out of 35. The dysfunctions regressed and these patients were able to enjoy satisfactory sexual activity.
Conclusion: Addictive masturbation, often accompanied by a dependency on cyber-pornography, has been seen to play a role in the etiology of certain types of erectile dysfunction or coital anejaculation. It is important to systematically identify the presence of these habits rather than conduct a diagnosis by elimination, in order to include habit-breaking deconditioning techniques in managing these dysfunctions.
6) How difficult is it to treat delayed ejaculation within a short-term psychosexual model? A case study comparison (2017) – A report on two “composite cases” illustrating the causes and treatments for delayed ejaculation (anorgasmia). “Patient B” represented several young men treated by the therapist. Interestingly, the paper states that Patient B’s “porn use had escalated into harder material”, “as is often the case”. The paper says that porn-related delayed ejaculation is not uncommon, and on the rise. The author calls for more research on porn’s effects of sexual functioning. Patient B’s delayed ejaculation was healed after 10 weeks of no porn. Excerpts:
The cases are composite cases taken from my work within the National Health Service in Croydon University Hospital, London. With the latter case (Patient B), it is important to note that the presentation reflects a number of young males who have been referred by their GPs with a similar diagnosis. Patient B is a 19-year-old who presented because he was unable to ejaculate via penetration. When he was 13, he was regularly accessing pornography sites either on his own through internet searches or via links that his friends sent him. He began masturbating every night while searching his phone for image…If he did not masturbate he was unable to sleep. The pornography he was using had escalated, as is often the case (see Hudson-Allez, 2010), into harder material (nothing illegal)…
We agreed that he would no longer use pornography to masturbate. This meant leaving his phone in a different room at night. We agreed that he would masturbate in a different way….
Patient B was able to achieve orgasm via penetration by the fifth session; the sessions are offered fortnightly in Croydon University Hospital so session five equates to approximately 10 weeks from consultation. He was happy and greatly relieved. In a three-month follow-up with Patient B, things were still going well.
Patient B is not an isolated case within the National Health Service (NHS) and in fact young men in general accessing psychosexual therapy, without their partners, speaks in itself to the stirrings of change.
7) Situational Psychogenic Anejaculation: A Case Study (2014) – The details reveal a case of porn-induced anejaculation. The husband’s only sexual experience prior to marriage was frequent masturbation to pornography – where he was able to ejaculate. He also reported sexual intercourse as less arousing than masturbation to porn. The key piece of information is that “re-training” and psychotherapy failed to heal his anejaculation. When those interventions failed, therapists suggested a complete ban on masturbation to porn. Eventually this ban resulted in successful sexual intercourse and ejaculation with a partner for the first time in his life. A few excerpts:
A is a 33-year-old married male with heterosexual orientation, a professional from a middle socio-economic urban background. He has had no premarital sexual contacts. He watched pornography and masturbated frequently. His knowledge about sex and sexuality was adequate. Following his marriage, Mr. A described his libido as initially normal, but later reduced secondary to his ejaculatory difficulties. Despite thrusting movements for 30-45 minutes, he had never been able to ejaculate or achieve orgasm during penetrative sex with his wife.
What didn’t work:
Mr. A’s medications were rationalized; clomipramine and bupropion were discontinued, and sertraline was maintained at a dose of 150 mg per day. Therapy sessions with the couple were held weekly for the initial few months, following which they were spaced to fortnightly and later monthly. Specific suggestions including focusing on sexual sensations and concentrating on the sexual experience rather than ejaculation were used to help reduce performance anxiety and spectatoring. Since problems persisted despite these interventions, intensive sex therapy was considered.
Eventually they instituted a complete ban on masturbation (which means he continued to masturbate to porn during the above failed interventions):
A ban on any form of sexual activity was suggested. Progressive sensate focus exercises (initially non-genital and later genital) were initiated. Mr. A described an inability to experience the same degree of stimulation during penetrative sex as compared to that which he experienced during masturbation. Once the ban on masturbation was enforced, he reported an increased desire for sexual activity with his partner.
After an unspecified amount of time, the ban on masturbation to porn lead to success:
Meanwhile, Mr. A and his wife decided to go ahead with Assisted Reproductive Techniques (ART) and underwent two cycles of intrauterine insemination. During a practice session, Mr. A ejaculated for the first time, following which he has been able to ejaculate satisfactorily during a majority of the couple’s sexual interactions.
8) Hidden in Shame: Heterosexual Men’s Experiences of Self-Perceived Problematic Pornography Use (2019) – Interviews of 15 male porn users. Several of the men reported porn addiction, escalation of use and porn-induced sexual problems. Excerpts relevant to porn-induced sexual dysfunctions, including Michael, who significantly improved his erectile function during sexual encounters by severely limiting his porn use:
Some men talked about seeking professional help to address their problematic pornography use. Such attempts at help-seeking had not been productive for the men, and at times even exacerbated feelings of shame. Michael, a university student who used pornography primarily as a coping mechanism for study-related stress, was having issues with erectile dysfunction during sexual encounters with women and sought help from his General Practitioner Doctor (GP):
Michael: When I went to the doctor at 19 [. . .], he prescribed Viagra and said [my issue] was just performance anxiety. Sometimes it worked, and sometimes it didn’t. It was personal research and reading that showed me the issue was porn [. . .] If I go to the doctor as a young kid and he prescribes me the blue pill, then I feel like no one is really talking about it. He should be asking about my porn use, not giving me Viagra. (23, Middle-Eastern, Student)
As a result of his experience, Michael never went back to that GP and started doing his own research online. He eventually found an article discussing a man approximately his age describing a similar type of sexual dysfunction, which caused him to consider pornography as a potential contributor. After making a concerted effort to lower his pornography use, his erectile dysfunction issues began to improve. He reported that even though his total frequency of masturbation did not reduce, he only watched pornography for about half of those instances. By halving the amount of times he combined masturbation with pornography, Michael said he was able to significantly improve his erectile function during sexual encounters with women.
9) Pornography Induced Erectile Dysfunction Among Young Men (2019) – Abstract:
This paper explores the phenomenon of pornography induced erectile dysfunction (PIED), meaning sexual potency problems in men due to Internet pornography consumption. Empirical data from men who suffer from this condition have been collected. A combination of topical life history method (with qualitative asynchronous online narrative interviews) and personal online diaries has been employed. The data have been analyzed using theoretical interpretative analysis (according to McLuhan’s media theory), based on analytic induction. The empirical investigation indicates that there is a correlation between pornography consumption and erectile dysfunction that suggests causation. The findings are based on 11 interviews along with two video diaries and three text diaries. The men are between the ages of 16 and 52; they report that an early introduction to pornography (usually during adolescence) is followed by daily consumption until a point is reached where extreme content (involving, for example, elements of violence) is needed to maintain arousal. A critical stage is reached when sexual arousal is exclusively associated with extreme and fast-paced pornography, rendering physical intercourse bland and uninteresting. This results in an inability to maintain an erection with a real-life partner, at which point the men embark on a “re-boot” process, giving up pornography. This has helped some of the men to regain their ability to achieve and sustain an erection.
Introduction to the results section:
Having processed the data, I have noticed certain patterns and recurring themes, following a chronological narrative in all of the interviews. These are: Introduction. One is first introduced to pornography, usually before puberty. Building a habit. One begins to consume pornography regularly. Escalation. One turns to more “extreme” forms of pornography, content-wise, in order to achieve the same effects previously achieved through less “extreme” forms of pornography. Realization. One notices sexual potency problems believed to be caused by pornography use. “Re-boot” process. One tries to regulate pornography use or eliminate it completely in order to regain one’s sexual potency. The data from the interviews are presented based on the above outline.
10) How Abstinence Affects Preferences (2016) [preliminary results] – Excerpts from the article:
Results of the First Wave – Main Findings
- The length of the longest streak participants performed before taking part in the survey correlates with time preferences. The second survey will answer the question if longer periods of abstinence render participants more able to delay rewards, or if more patient participants are more likely to perform longer streaks.
- Longer periods of abstinence most likely cause less risk aversion (which is good). The second survey will provide the final proof.
- Personality correlates with length of streaks. The second wave will reveal if abstinence influences personality or if personality can explain variation in the length of streaks.
Results of the Second Wave – Main Findings
- Abstaining from pornography and masturbation increases the ability to delay rewards
- Participating in a period of abstinence renders people more willing to take risks
- Abstinence renders people more altruistic
- Abstinence renders people more extroverted, more conscientious, and less neurotic
DAVID LEY: “Numerous studies have now demonstrated that high porn-users tend to be people with higher libido“
RESPONSE: There’s a reason Ley provides no citation. Study after study refutes this often repeated Ley meme.
Ley’s “higher libido” claim appears to based on his blog post with the catchy title: “Your Brain on Porn – It’s NOT Addictive”. The Ley blog post is not about the science behind YBOP. Instead, it’s about a single EEG study, whose lead author is his colleague Nicole Prause: (Steele et al. 2013). Both Ley and Prause claimed that the study’s findings support the premise that porn/sex addiction is nothing more than “high sexual desire.”
Contrary to claims by Ley and Prause, Steele et al. reported greater cue-reactivity to porn correlating with LESS desire for sex with a partner (but not lower desire to masturbate to porn). To put it another way – individuals with more brain activation and cravings for porn would rather masturbate to porn than have sex with a real person. This is not an indication of “high sexual desire.”
Greater cue reactivity to porn coupled with lower desire for sex with real partners aligns the 2014 Cambridge University brain study on porn addicts. The actual findings of Steele et al., 2013 do not support its conclusion, or Ley’s blog post assertions. Eight subsequent peer-reviewed papers say that the Steele et al. findings actually lend support to the porn addiction model (as opposed to the “high sexual desire” hypothesis): Peer-reviewed critiques of Steele et al., 2013
In 2015, Nicole Prause published a second EEG study, which found LESS neural response (with brief exposure to still images) in “porn addicts” when compared to controls (Steele et al., 2013 had no control subjects) This is evidence of abnormally reduced desire in porn addicts. These findings align perfectly with Kühn & Gallinat (2014), which found that more porn use correlated with less brain activation in response to pictures of vanilla porn. In other words, “porn addicts” were desensitized and – far from having high sexual desire – needed greater stimulation than non-addicts to be turned on. Put simply, the results of Prause’s second EEG study indicate LESS sexual arousal – not higher sexual desire. Nine peer-reviewed papers all agree that Prause et al., 2015 actually found desensitization/habituation in frequent porn users: Peer-reviewed critiques of Prause et al., 2015
In fact, Prause stated in this recent Quora post that she no longer believes that “sex addicts” have high libidos:
“I was partial to the high sex drive explanation, but this LPP study we just published is persuading me to be more open to sexual compulsivity.”
Since Prause has flip-flopped, where is Ley’s support for the “porn/sex addiction = high libido” claim? Below are multiple studies that tested, and falsified, David Ley’s “high libido = sex/porn addiction” claim entirely:
1) “Is High Sexual Desire a Facet of Male Hypersexuality? Results from an Online Study.” (2015) – Researchers found virtually no overlap between the men with hypersexuality and the men with “High Sexual Desire”. Excerpt from the paper:
“The study findings point to a distinct phenomenology of High Sexual Desire and Hypersexuality in men.”
2) “Hypersexuality and High Sexual Desire: Exploring the Structure of Problematic Sexuality” (2015) – The study found little overlap between high sexual desire and hypersexuality. Excerpt from the paper:
“Our study supports the distinctiveness of hypersexuality and high sexual desire/activity.”
3) “Neural Correlates of Sexual Cue Reactivity in Individuals with and without Compulsive Sexual Behaviours” (2014) – A Cambridge University fMRI study comparing porn addicts to healthy controls. The study found that porn addicts had lower sexual desire and greater difficulty achieving erections, yet had greater cue-reactivity to porn (similar to Steele et al. above). Excerpts from the paper:
“On an adapted version of the Arizona Sexual Experiences Scale [43], CSB subjects compared to healthy volunteers had significantly more difficulty with sexual arousal and experienced more erectile difficulties in intimate sexual relationships but not to sexually explicit material (Table S3 in File S1).”
CSB subjects reported that as a result of excessive use of sexually explicit materials….. experienced diminished libido or erectile function specifically in physical relationships with women (although not in relationship to the sexually explicit material)…
4) “Patient Characteristics by Type of Hypersexuality Referral: A Quantitative Chart Review of 115 Consecutive Male Cases” (2015) – Study on men with hypersexuality disorders. 27 were classified as “avoidant masturbators,” meaning they masturbated to porn one or more hours per day or more than 7 hours per week. 71% of the compulsive porn users reported sexual functioning problems, with 33% reporting delayed ejaculation.
5) “Erectile Dysfunction, Boredom, and Hypersexuality among Coupled Men from Two European Countries” (2015) – This survey reported a strong correlation between erectile dysfunction and measures of hypersexuality. Excerpt:
“Hypersexuality was significantly correlated with proneness to sexual boredom and more problems with erectile function.”
6) “Adolescents and web porn: a new era of sexuality (2015)” – This Italian study analyzed the effects of Internet porn on high school seniors, co-authored by urology professor Carlo Foresta, president of the Italian Society of Reproductive Pathophysiology. The most interesting finding is that 16% of those who consume porn more than once a week report abnormally low sexual desire compared with 0% in non-consumers (and 6% for those who consume less than once a week). From the study:
“21.9% define it as habitual, 10% report that it reduces sexual interest towards potential real-life partners, and the remaining, 9.1% report a kind of addiction. In addition, 19% of overall pornography consumers report an abnormal sexual response, while the percentage rose to 25.1% among regular consumers.”
7) “Brain Structure and Functional Connectivity Associated With Pornography Consumption: The Brain on Porn” (2014) – A Max Planck study which found 3 significant addiction-related brain changes correlating with the amount of porn consumed. It also found that the more porn consumed the less reward circuit activity in response to brief exposure (.530 second) to vanilla porn. In a 2014 article lead author Simone Kühn said:
“We assume that subjects with a high porn consumption need increasing stimulation to receive the same amount of reward. That could mean that regular consumption of pornography more or less wears out your reward system. That would fit perfectly the hypothesis that their reward systems need growing stimulation.”
A more technical description of this study from a review of the literature by Kuhn & Gallinat – Neurobiological Basis of Hypersexuality (2016).
“The more hours participants reported consuming pornography, the smaller the BOLD response in left putamen in response to sexual images. Moreover, we found that more hours spent watching pornography was associated with smaller gray matter volume in the striatum, more precisely in the right caudate reaching into the ventral putamen. We speculate that the brain structural volume deficit may reflect the results of tolerance after desensitization to sexual stimuli.”
8) “Unusual masturbatory practice as an etiological factor in the diagnosis and treatment of sexual dysfunction in young men” (2014) – One of the 4 case studies in this paper reports on a man with porn-induced sexual problems (low libido, fetishes, anorgasmia). The sexual intervention called for a 6-week abstinence from porn and masturbation. After 8 months the man reported increased sexual desire, successful sex and orgasm, and enjoying “good sexual practices.”
9) “Pornography use: who uses it and how it is associated with couple outcomes” (2012) – While not a study on “hypersexuals”, it reported that 1) porn use was consistently correlated with low scores on sexual satisfaction, and 2) that there was no differences in sexual desire between the porn users and the non-users.
10) Sexual Desire, not Hypersexuality, is Related to Neurophysiological Responses Elicited by Sexual Images (2013) -This EEG study was touted in the media as evidence against the existence of porn/sex addiction. Not so. Steele et al. 2013 actually lends support to the existence of both porn addiction and porn use down-regulating sexual desire. How so? The study reported higher EEG readings (relative to neutral pictures) when subjects were briefly exposed to pornographic photos. Studies consistently show that an elevated P300 occurs when addicts are exposed to cues (such as images) related to their addiction.
In line with the Cambridge University brain scan studies, this EEG study also reported greater cue-reactivity to porn correlating with less desire for partnered sex. To put it another way – individuals with greater brain activation to porn would rather masturbate to porn than have sex with a real person. Shockingly, study spokesperson Nicole Prause claimed that porn users merely had “high libido,” yet the results of the study say the exact opposite (subjects’ desire for partnered sex was dropping in relation to their porn use).
Together these two Steele et al. findings indicate greater brain activity to cues (porn images), yet less reactivity to natural rewards (sex with a person). That”s sensitization & desensitization, which are hallmarks of an addiction. 8 peer-reviewed papers explain the truth: Peer-reviewed critiques of Steele et al., 2013 Also see this extensive YBOP critique.
11) Modulation of Late Positive Potentials by Sexual Images in Problem Users and Controls Inconsistent with “Porn Addiction” (2015) -A second EEG study from Nicole Prause’s team. This study compared the 2013 subjects from Steele et al., 2013 to an actual control group (yet it suffered from the same methodological flaws named above). The results: Compared to controls “individuals experiencing problems regulating their porn viewing” had lower brain responses to one-second exposure to photos of vanilla porn. The lead author claims these results “debunk porn addiction.” What legitimate scientist would claim that their lone anomalous study has debunked a well established field of study?
In reality, the findings of Prause et al. 2015 align perfectly with Kühn & Gallinat (2014), which found that more porn use correlated with less brain activation in response to pictures of vanilla porn. Prause et al. findings also align with Banca et al. 2015 which is #13 in this list. Moreover, another EEG study found that greater porn use in women correlated with less brain activation to porn. Lower EEG readings mean that subjects are paying less attention to the pictures. Put simply, frequent porn users were desensitized to static images of vanilla porn. They were bored (habituated or desensitized). See this extensive YBOP critique. 9 peer-reviewed papers agree that this study actually found desensitization/habituation in frequent porn users (consistent with addiction): Peer-reviewed critiques of Prause et al., 2015
Prause proclaimed that her EEG readings assessed “cue-reactivity” (sensitization), rather than habituation. Even if Prause were correct she conveniently ignores the gaping hole in her “falsification” assertion: Even if Prause et al. 2015 had found less cue-reactivity in frequent porn users, 25 other neurological studies have reported cue-reactivity or cravings (sensitization) in compulsive porn users: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21 , 22, 23, 24, 25. Science doesn’t go with the lone anomalous study hampered by serious methodological flaws; science goes with the preponderance of evidence (unless you are agenda-driven).
12) Use of pornography in a random sample of Norwegian heterosexual couples (2009) – Porn use was correlated with more sexual dysfunctions in the man and negative self perception in the female. The couples who did not use porn had no sexual dysfunctions. A few excerpts from the study:
In couples where only one partner used pornography, we found more problems related to arousal (male) and negative (female) self-perception.
The couples who did not use pornography… may be considered more traditional in relation to the theory of sexual scripts. At the same time, they did not seem to have any dysfunctions.
13) Masturbation and Pornography Use Among Coupled Heterosexual Men With Decreased Sexual Desire: How Many Roles of Masturbation? (2015) – Masturbating to porn was related with decreased sexual desire and low relationship intimacy. Excerpts:
“Among men who masturbated frequently, 70% used pornography at least once a week. A multivariate assessment showed that sexual boredom, frequent pornography use, and low relationship intimacy significantly increased the odds of reporting frequent masturbation among coupled men with decreased sexual desire.”
“Among men [with decreased sexual desire] who used pornography at least once a week [in 2011], 26.1% reported that they were unable to control their pornography use. In addition, 26.7% of men reported that their use of pornography negatively affected their partnered sex and 21.1% claimed to have attempted to stop using pornography.”
14) Men’s Sexual Life and Repeated Exposure to Pornography. A New Issue? (2015) – Excerpts:
Mental health specialists should take in consideration the possible effects of pornography consumption on men sexual behaviors, men sexual difficulties and other attitudes related to sexuality. In the long term pornography seems to create sexual dysfunctions, especially the individual’s inability to reach an orgasm with his partner. Someone who spends most of his sexual life masturbating while watching porn engages his brain in rewiring its natural sexual sets so that it will soon need visual stimulation to achieve an orgasm.
Many different symptoms of porn consumption, such as the need to involve a partner in watching porn, the difficulty in reaching orgasm, the need for porn images in order to ejaculate turn into sexual problems. These sexual behaviors may go on for months or years and it may be mentally and bodily associated with the erectile dysfunction, although it is not an organic dysfunction. Because of this confusion, which generates embarrassment, shame and denial, lots of men refuse to encounter a specialist
Pornography offers a very simple alternative to obtain pleasure without implying other factors that were involved in human’s sexuality along the history of mankind. The brain develops an alternative path for sexuality which excludes “the other real person” from the equation. Furthermore, pornography consumption in a long term makes men more prone to difficulties in obtaining an erection in a presence of their partners.
Further, we found no associations between the CSBI Control scale and the BIS-BAS. This would indicate that lack of sexual behavior control is related to specific sexual excitation and inhibitory mechanisms and not to more general behavioral activation and inhibitory mechanisms. This would seem to support conceptualizing hypersexuality as a dysfunction of sexuality as proposed by Kafka. Further, it does not appear that hypersexuality is a manifestation of high sex drive, but that it involves high excitation and a lack of inhibitory control, at least with respect to inhibition owing to expected negative outcomes.
16) Hypersexual, Sexually Compulsive, or Just Highly Sexually Active? Investigating Three Distinct Groups of Gay and Bisexual Men and Their Profiles of HIV-Related Sexual Risk (2016) – If high sexual desire and sex addiction were the same, there would only be one group of individuals per population. This study, like the ones above, reported several distinct sub-groups, yet all groups reported similar rates of sexual activity.
Emerging research supports the notion that sexual compulsivity (SC) and hypersexual disorder (HD) among gay and bisexual men (GBM) might be conceptualized as comprising three groups—Neither SC nor HD; SC only, and Both SC and HD—that capture distinct levels of severity across the SC/HD continuum.
Nearly half (48.9 %) of this highly sexually active sample was classified as Neither SC nor HD, 30 % as SC Only, and 21.1 % as Both SC and HD. While we found no significant differences between the three groups on reported number of male partners, anal sex acts, or anal sex acts
17) The effects of sexually explicit material use on romantic relationship dynamics (2016) – As with many other studies, solitary porn users report poorer relationship and sexual satisfaction. Employing the Pornography Consumption Effect Scale (PCES), the study found that higher porn use was related to poorer sexual function, more sexual problems, and a “worse sex life”. An excerpt describing the correlation between the PCES “Negative Effects” on “Sex Life” questions and frequency of porn use:
There were no significant differences for the Negative Effect Dimension PCES across the frequency of sexually explicit material use; however, there were significant differences on the Sex Life subscale where High Frequency Porn Users reported greater negative effects than Low Frequency Porn Users.
18) Male masturbation habits and sexual dysfunctions (2016) – It’s by a French psychiatrist who is the current president of the European Federation of Sexology. While the abstract shifts back and forth between Internet pornography use and masturbation, it’s clear that he’s mostly referring to porn-induced sexual dysfunctions (erectile dysfunction and anorgasmia). The paper revolves around his clinical experience with 35 men who developed erectile dysfunction and/or anorgasmia, and his therapeutic approaches to help them. The author states that most of his patients used porn, with several being addicted to porn. The abstract points to internet porn as the primary cause of the problems (keep in mind that masturbation does not cause chronic ED, and it is never given as a cause of ED). Excerpts:
Intro: Harmless and even helpful in his usual form widely practiced, masturbation in its excessive and pre-eminent form, generally associated today to pornographic addiction, is too often overlooked in the clinical assessment of sexual dysfunction it can induce.
Results: Initial results for these patients, after treatment to “unlearn” their masturbatory habits and their often associated addiction to pornography, are encouraging and promising. A reduction in symptoms was obtained in 19 patients out of 35. The dysfunctions regressed and these patients were able to enjoy satisfactory sexual activity.
Conclusion: Addictive masturbation, often accompanied by a dependency on cyber-pornography, has been seen to play a role in the etiology of certain types of erectile dysfunction or coital anejaculation. It is important to systematically identify the presence of these habits rather than conduct a diagnosis by elimination, in order to include habit-breaking deconditioning techniques in managing these dysfunctions.
19) The Dual Control Model – The Role Of Sexual Inhibition & Excitation In Sexual Arousal And Behavior (2007) – Newly rediscovered and very convincing. In an experiment employing video porn, 50% of the young men couldn’t become aroused or achieve erections with porn (average age was 29). The shocked researchers discovered that the men’s erectile dysfunction was,
“related to high levels of exposure to and experience with sexually explicit materials.“
The men experiencing erectile dysfunction had spent a considerable amount of time in bars and bathhouses where porn was “omnipresent,” and “continuously playing“. The researchers stated:
“Conversations with the subjects reinforced our idea that in some of them a high exposure to erotica seemed to have resulted in a lower responsivity to “vanilla sex” erotica and an increased need for novelty and variation, in some cases combined with a need for very specific types of stimuli in order to get aroused.”
20) Online sexual activities: An exploratory study of problematic and non-problematic usage patterns in a sample of men (2016) – This Belgian study from a leading research university found problematic Internet porn use was associated with reduced erectile function and reduced overall sexual satisfaction. Yet problematic porn users experienced greater cravings. The study appears to report escalation, as 49% of the men viewed porn that “was not previously interesting to them or that they considered disgusting.” (See studies reporting habituation/desensitization to porn and escalation of porn use) Excerpts:
“This study is the first to directly investigate the relationships between sexual dysfunctions and problematic involvement in OSAs. Results indicated that higher sexual desire, lower overall sexual satisfaction, and lower erectile function were associated with problematic OSAs (online sexual activities). These results can be linked to those of previous studies reporting a high level of arousability in association with sexual addiction symptoms (Bancroft & Vukadinovic, 2004; Laier et al., 2013; Muise et al., 2013).”
In addition, we finally have a study that asks porn users about possible escalation to new or disturbing porn genres. Guess what it found?
“Forty-nine percent mentioned at least sometimes searching for sexual content or being involved in OSAs that were not previously interesting to them or that they considered disgusting, and 61.7% reported that at least sometimes OSAs were associated with shame or guilty feelings.”
Note – This is the first study to directly investigate the relationships between sexual dysfunctions and problematic porn use. Two other studies claiming to have investigated correlations between porn use and erectile functioning cobbled together data from earlier studies in an unsuccessful attempt to debunk porn-induced ED. Both were criticized in the peer-reviewed literature: paper 1 was not an authentic study, and has been thoroughly discredited; paper 2 actually found correlations that support porn-induced ED. Moreover, paper 2 was only a “brief communication” that did not report important data.
21) Altered Appetitive Conditioning and Neural Connectivity in Subjects With Compulsive Sexual Behavior (2016) – “Compulsive Sexual Behaviors” (CSB) means the men were porn addicts, because CSB subjects averaged nearly 20 hours of porn use per week. The controls averaged 29 minutes per week. Interestingly, 3 of the 20 CSB subjects mentioned to interviewers that they suffered from “orgasmic-erection disorder,” while none of the control subjects reported sexual problems.
22) Study sees link between porn and sexual dysfunction (2017) – The findings of an upcoming study presented at the American Urological Association’s annual meeting. A few excerpts:
Young men who prefer pornography to real-world sexual encounters might find themselves caught in a trap, unable to perform sexually with other people when the opportunity presents itself, a new study reports. Porn-addicted men are more likely to suffer from erectile dysfunction and are less likely to be satisfied with sexual intercourse, according to survey findings presented Friday at the American Urological Association’s annual meeting, in Boston.
23) “I think it has been a negative influence in many ways but at the same time I can’t stop using it”: Self-identified problematic pornography use among a sample of young Australians (2017) – Online survey of Australians, aged 15-29. Those who had ever viewed pornography (n=856) were asked in an open-ended question: ‘How has pornography influenced your life?’.
Among participants who responded to the open-ended question (n=718), problematic usage was self-identified by 88 respondents. Male participants who reported problematic usage of pornography highlighted effects in three areas: on sexual function, arousal and relationships. Responses included “I think it has been a negative influence in many ways but at the same time I can’t stop using it” (Male, Aged 18–19).
24) Exploring the Relationship Between Erotic Disruption During the Latency Period and the Use of Sexually Explicit Material, Online Sexual Behaviors, and Sexual Dysfunctions in Young Adulthood (2009) – Study examined correlations between current porn use (sexually explicit material – SEM) and sexual dysfunctions, and porn use during “latency period” (ages 6-12) and sexual dysfunctions. The average age of participants was 22. While current porn use correlated with sexual dysfunctions, porn use during latency (ages 6-12) had an even stronger correlation with sexual dysfunctions. A few excerpts:
Findings suggested that latency erotic disruption by way of sexually explicit material (SEM) and/or child sexual abuse may be associated to adult online sexual behaviors.
Furthermore, results demonstrated that latency SEM exposure was a significant predictor of adult sexual dysfunctions.
We hypothesized that exposure to latency SEM exposure would predict adult use of SEM. Study findings supported our hypothesis, and demonstrated that latency SEM exposure was a statistically significant predictor of adult SEM use. This suggested that individuals who were exposed to SEM during latency, may continue this behavior into adulthood. Study findings also indicated that latency SEM exposure was a significant predictor of adult online sexual behaviors.
In short, the evidence is piling up that internet porn erodes normal sexual desire, leaving users less responsive to pleasure. They may crave porn, but that is more likely evidence of an addiction-related brain change known as “sensitization” (hyper-reactivity to addiction-related cues). Cravings certainly cannot be assumed to be evidence of greater libido.
DAVID LEY: “It is most likely that these dispositions correlate with neurological characteristics, which these studies are finding. In other words, these neurological characteristics are in fact the cause, not the effect.”
RESPONSE: Without a shred of evidence or a single example, Ley is claiming that the brain changes found the 50 studies addiction must have existed before porn use. In reality, the two main addiction-related brain changes reported by the studies can only develop from chronic use:
- Sensitization: Chronic use leads to altered nerve connections which cause the reward circuitry to buzz in response to addiction-related cues or thoughts. This Pavlovian memory is what induces severe cravings that make the addiction far more compelling than other activities in the addict’s life. (Studies reporting sensitization in internet porn users: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25.)
- Desensitization: Chronic use leads to the individual becoming less sensitive to pleasure, which often manifests as the need for greater and greater stimulation to achieve the same buzz. This is referred to as tolerance and only occurs with chronic use. (Studies reporting desensitization in porn users: 1, 2, 3, 4, 5, 6, 7, 8.)
It’s quite telling that Ley is incapable of naming these “neurological characteristics.” Reality: The mechanisms of addiction have been studied for nearly 60 years. The very specific brain changes caused by addiction have been elucidated down to the cellular, protein, and epigenetic levels. These brain changes have been correlated over and over with the behaviors collectively known as the “addiction phenotype.” Addiction-like behaviors can be induced in animals simply by increasing a single protein within the reward center (Deltafosb). In short, a lot is known about the biology of addiction – more than any other mental disorder – even if it remains unknown to Dr. Ley.
Four major brain changes are involved with both drug and behavioral addictions, as outlined in this paper published this year in The New England Journal of Medicine: “Neurobiologic Advances from the Brain Disease Model of Addiction (2016)“. This landmark review by the Director of the National Institute on Alcohol Abuse and Alcoholism (NIAAA) George F. Koob, and the director of the National Institute on Drug Abuse (NIDA) Nora D. Volkow, not only outlines the brain changes involved in addiction, it also states in its opening paragraph that sex addiction exists:
“We conclude that neuroscience continues to support the brain disease model of addiction. Neuroscience research in this area not only offers new opportunities for the prevention and treatment of substance addictions and related behavioral addictions (e.g., to food, sex, and gambling)….”
In simple, and very broad, terms the major fundamental brain changes are: 1) Sensitization, 2) Desensitization, 3) Hypofrontality/Dysfunctional prefrontal circuits 4) Dysfunctional stress circuits. All 4 of these brain changes have been identified among the 44 neuroscience studies on porn users:
- Studies reporting sensitization (cue-reactivity & cravings) in porn users/sex addicts: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25.
- Studies reporting desensitization or habituation (resulting in tolerance) in porn users/sex addicts: 1, 2, 3, 4, 5, 6, 7, 8.
- Studies reporting poorer executive functioning (hypofrontality) or altered prefrontal activity in porn users/sex addicts: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17.
- Studies indicating a dysfunctional stress system in porn users/sex addicts: 1, 2, 3, 4, 5.
I find it interesting that Dr. Ley seems to always claim that there’s no scientific support for porn addiction, yet not only do 50 studies provide support for porn/sex addiction, the world’s top addiction experts do also. The little bubble he has constructed, where porn addiction cannot possibly exist, is seriously out of step with science.
DAVID LEY: “Grubbs also found recently that the identity of “porn addict” is an iatrogenic concept, which creates harm and distress, by telling an individual to hate and fear their own sexuality“
RESPONSE: Nothing could farther from the truth. Here is an extensive analysis of Grubbs’s study – Critique of “Perceived Addiction to Internet Pornography and Psychological Distress: Examining Relationships Concurrently and Over Time” (2015).
Both Ley’s and the Grubbs study’s claims depend upon two false premises:
- That Grubbs’s porn addiction test (CPUI) assesses “perceived porn addiction” rather than actual addiction. It does not. Grubbs et al. re-labeled Grubbs’s self-created porn addiction test as a “perceived porn addiction” test. However, this Cyber Pornography Use Inventory (CPUI) questionnaire is in fact similar to many other drug and behavioral addiction questionnaires. Like other addiction tests, the CPUI assesses behaviors and symptoms common to all addictions, such as: the inability to control use; compulsion to use, cravings to use, negative psychological, social and emotional effects; and preoccupation with using. In fact, only 1 of its 9 questions even hints at “perceived addiction.” Yet we are told that a person’s total score for all 9 questions is synonymous with “perceived addiction” rather than addiction itself. Very misleading, very clever, and without any scientific basis.
- That Grubbs found little correlation between CPUI scores and hours of porn use. Contrary to Ley’s claim, Grubbs found a pretty strong correlation between hours of use and the CPUI! From p. 6 of the study:
“Additionally, average daily pornography use in hours was significantly and positively associated with depression, anxiety, and anger, as well as with perceived addiction.”
Stop the presses! This excerpt directly contradicts all the headlines, which claim that pornography use was NOT strongly correlated with psychological distress or “perceived addiction.” Again, whenever you see the phrase “perceived addiction” it actually denotes the subjects’ total score on the CPUI (which is a porn addiction test). Really get this: The Grubbs study did NOT assess “perceived addiction.” There are many more details in this critique that debunks assertions put forth in lay articles and the claims made within the Grubbs’s studies: Is Joshua Grubbs pulling the wool over our eyes with his “perceived porn addiction” research? (2016).
Update: Joshua Grubbs published a study testing the talking point that religious people are more likely to believe they are addicted to porn (even though the Grubbs studies never assessed “belief in being addicted porn”). Faced with thoughtful skepticism about his assumptions, and reservations about the unfounded claims that his CPUI-9 instrument could indeed distinguish “perceived pornography addiction” from genuine problematic porn use, Dr. Grubbs did the right thing as a scientist. He pre-registered a study to test his hypotheses/assumptions directly. Pre-registration is a sound scientific practice that prevents researchers from changing hypotheses after collecting data.
The results contradicted both his earlier conclusions and the meme (“porn addiction is just shame”) that the press helped to popularize.
Dr. Grubbs set out to prove that religiosity was the main predictor of “believing yourself addicted to porn.” He and his team of researchers surveyed 3 rather large, diverse samples (male, female, etc.): Who’s a Porn Addict? Examining the Roles of Pornography Use, Religiousness, and Moral Incongruence. (He posted the results online, although his team’s paper has not yet been formally published).
This time, however, he didn’t rely on his CPUI-9 instrument. (The CPUI-9 includes 3 “guilt and shame/emotional distress” questions not normally found in addiction instruments – and which skew its results, causing religious porn users to score higher and non-religious users to score lower than subjects do on standard addiction-assessment instruments.) Instead, the Grubbs team asked 2 direct yes/no questions of porn users (“I believe that I am addicted to internet pornography.” “I would call myself an internet pornography addict.”), and compared results with scores on a “moral disapproval” questionnaire.
Directly contradicting his earlier claims, Dr. Grubbs and his research team found that believing you are addicted to porn correlates most strongly with daily hours of porn use, not with religiousness. As noted above, some of Grubbs studies also found that hours of use was a stronger predictor of “perceived addiction” than religiosity. From the new study’s abstract:
In contrast to prior literature indicating that moral incongruence and religiousness are the best predictors of perceived addiction [using the CPUI-9], results from all three samples indicated that male gender and pornography use behaviors were the most strongly associated with self-identification as a pornography addict.
Based on their results, Dr. Grubbs and his co-authors advise that,
“mental and sexual health professionals should take the concerns of clients identifying as pornography addicts seriously.”
DAVID LEY: “There has not been a single peer-reviewed paper published which demonstrate any evidence that ED related to porn use is a real phenomenon.“
RESPONSE: Absolutely false. And it’s not just erectile dysfunction. Several studies have found relationships between porn use in young men and ED, anorgamsia, low sexual desire, delayed ejaculation and lower brain activation to sexual images. In addition this page contains articles and videos by over 100 experts (urology professors, urologists, psychiatrists, psychologists, sexologists, MDs) who acknowledge and have successfully treated porn-induced ED and porn-induced loss of sexual desire.
Studies reporting links between porn use/sex addiction and ED, anorgamsia, low sexual desire, delayed ejaculation, and lower brain activation to sexual images.
In addition to the studies below, this page contains articles and videos by over 130 experts (urology professors, urologists, psychiatrists, psychologists, sexologists, MDs) who acknowledge and have successfully treated porn-induced ED and porn-induced loss of sexual desire. The first 7 studies demonstrate causation as participants eliminated porn use and healed chronic sexual dysfunctions:
1) Is Internet Pornography Causing Sexual Dysfunctions? A Review with Clinical Reports (2016) – An extensive review of the literature related to porn-induced sexual problems. Involving 7 US Navy doctors, the review provides the latest data revealing a tremendous rise in youthful sexual problems. It also reviews the neurological studies related to porn addiction and sexual conditioning via Internet porn. The doctors provide 3 clinical reports of men who developed porn-induced sexual dysfunctions. Two of the three men healed their sexual dysfunctions by eliminating porn use. The third man experienced little improvement as he was unable to abstain from porn use. Excerpt:
Traditional factors that once explained men’s sexual difficulties appear insufficient to account for the sharp rise in erectile dysfunction, delayed ejaculation, decreased sexual satisfaction, and diminished libido during partnered sex in men under 40. This review (1) considers data from multiple domains, e.g., clinical, biological (addiction/urology), psychological (sexual conditioning), sociological; and (2) presents a series of clinical reports, all with the aim of proposing a possible direction for future research of this phenomenon. Alterations to the brain’s motivational system are explored as a possible etiology underlying pornography-related sexual dysfunctions. This review also considers evidence that Internet pornography’s unique properties (limitless novelty, potential for easy escalation to more extreme material, video format, etc.) may be potent enough to condition sexual arousal to aspects of Internet pornography use that do not readily transition to real-life partners, such that sex with desired partners may not register as meeting expectations and arousal declines. Clinical reports suggest that terminating Internet pornography use is sometimes sufficient to reverse negative effects, underscoring the need for extensive investigation using methodologies that have subjects remove the variable of Internet pornography use.
2) Male masturbation habits and sexual dysfunctions (2016) – It’s by a French psychiatrist who is the current president of the European Federation of Sexology. While the abstract shifts back and forth between Internet pornography use and masturbation, it’s clear that he’s mostly referring to porn-induced sexual dysfunctions (erectile dysfunction and anorgasmia). The paper revolves around his clinical experience with 35 men who developed erectile dysfunction and/or anorgasmia, and his therapeutic approaches to help them. The author states that most of his patients used porn, with several being addicted to porn. The abstract points to internet porn as the primary cause of the problems (keep in mind that masturbation does not cause chronic ED, and it is never given as a cause of ED). 19 of the 35 men saw significant improvements in sexual functioning. The other men either dropped out of treatment or are still trying to recover. Excerpts:
Intro: Harmless and even helpful in his usual form widely practiced, masturbation in its excessive and pre-eminent form, generally associated today to pornographic addiction, is too often overlooked in the clinical assessment of sexual dysfunction it can induce.
Results: Initial results for these patients, after treatment to “unlearn” their masturbatory habits and their often associated addiction to pornography, are encouraging and promising. A reduction in symptoms was obtained in 19 patients out of 35. The dysfunctions regressed and these patients were able to enjoy satisfactory sexual activity.
Conclusion: Addictive masturbation, often accompanied by a dependency on cyber-pornography, has been seen to play a role in the etiology of certain types of erectile dysfunction or coital anejaculation. It is important to systematically identify the presence of these habits rather than conduct a diagnosis by elimination, in order to include habit-breaking deconditioning techniques in managing these dysfunctions.
3) Unusual masturbatory practice as an etiological factor in the diagnosis and treatment of sexual dysfunction in young men (2014) – One of the 4 case studies in this paper reports on a man with porn-induced sexual problems (low libido, fetishes, anorgasmia). The sexual intervention called for a 6-week abstinence from porn and masturbation. After 8 months the man reported increased sexual desire, successful sex and orgasm, and enjoying “good sexual practices. This is the first peer-reviewed chronicling of a recovery from porn-induced sexual dysfunctions. Excerpts from the paper:
“When asked about masturbatory practices, he reported that in the past he had been masturbating vigorously and rapidly while watching pornography since adolescence. The pornography originally consisted mainly of zoophilia, and bondage, domination, sadism, and masochism, but he eventually got habituated to these materials and needed more hardcore pornography scenes, including transgender sex, orgies, and violent sex. He used to buy illegal pornographic movies on violent sex acts and rape and visualized those scenes in his imagination to function sexually with women. He gradually lost his desire and his ability to fantasize and decreased his masturbation frequency.”
In conjunction with weekly sessions with a sex therapist, the patient was instructed to avoid any exposure to sexually explicit material, including videos, newspapers, books, and internet pornography.
After 8 months, the patient reported experiencing successful orgasm and ejaculation. He renewed his relationship with that woman, and they gradually succeeded in enjoying good sexual practices.
4) How difficult is it to treat delayed ejaculation within a short-term psychosexual model? A case study comparison (2017) – A report on two “composite cases” illustrating the causes and treatments for delayed ejaculation (anorgasmia). “Patient B” represented several young men treated by the therapist. Interestingly, the paper states that Patient B’s “porn use had escalated into harder material”, “as is often the case”. The paper says that porn-related delayed ejaculation is not uncommon, and on the rise. The author calls for more research on porn’s effects of sexual functioning. Patient B’s delayed ejaculation was healed after 10 weeks of no porn. Excerpts:
The cases are composite cases taken from my work within the National Health Service in Croydon University Hospital, London. With the latter case (Patient B), it is important to note that the presentation reflects a number of young males who have been referred by their GPs with a similar diagnosis. Patient B is a 19-year-old who presented because he was unable to ejaculate via penetration. When he was 13, he was regularly accessing pornography sites either on his own through internet searches or via links that his friends sent him. He began masturbating every night while searching his phone for image…If he did not masturbate he was unable to sleep. The pornography he was using had escalated, as is often the case (see Hudson-Allez, 2010), into harder material (nothing illegal)…
Patient B was exposed to sexual imagery via pornography from the age of 12 and the pornography he was using had escalated to bondage and dominance by the age of 15.
We agreed that he would no longer use pornography to masturbate. This meant leaving his phone in a different room at night. We agreed that he would masturbate in a different way….
Patient B was able to achieve orgasm via penetration by the fifth session; the sessions are offered fortnightly in Croydon University Hospital so session five equates to approximately 10 weeks from consultation. He was happy and greatly relieved. In a three-month follow-up with Patient B, things were still going well.
Patient B is not an isolated case within the National Health Service (NHS) and in fact young men in general accessing psychosexual therapy, without their partners, speaks in itself to the stirrings of change.
This article therefore supports previous research that has linked masturbation style to sexual dysfunction and pornography to masturbation style. The article concludes by suggesting that the successes of psychosexual therapists in working with DE are rarely recorded in the academic literature, which has allowed the view of DE as a difficult disorder to treat remain largely unchallenged. The article calls for research into pornography usage and its effect on masturbation and genital desensitisation.
5) Situational Psychogenic Anejaculation: A Case Study (2014) – The details reveal a case of porn-induced anejaculation. The husband’s only sexual experience prior to marriage was frequent masturbation to pornography – where he was able to ejaculate. He also reported sexual intercourse as less arousing than masturbation to porn. The key piece of information is that “re-training” and psychotherapy failed to heal his anejaculation. When those interventions failed, therapists suggested a complete ban on masturbation to porn. Eventually this ban resulted in successful sexual intercourse and ejaculation with a partner for the first time in his life. A few excerpts:
A is a 33-year-old married male with heterosexual orientation, a professional from a middle socio-economic urban background. He has had no premarital sexual contacts. He watched pornography and masturbated frequently. His knowledge about sex and sexuality was adequate. Following his marriage, Mr. A described his libido as initially normal, but later reduced secondary to his ejaculatory difficulties. Despite thrusting movements for 30-45 minutes, he had never been able to ejaculate or achieve orgasm during penetrative sex with his wife.
What didn’t work:
Mr. A’s medications were rationalized; clomipramine and bupropion were discontinued, and sertraline was maintained at a dose of 150 mg per day. Therapy sessions with the couple were held weekly for the initial few months, following which they were spaced to fortnightly and later monthly. Specific suggestions including focusing on sexual sensations and concentrating on the sexual experience rather than ejaculation were used to help reduce performance anxiety and spectatoring. Since problems persisted despite these interventions, intensive sex therapy was considered.
Eventually they instituted a complete ban on masturbation (which means he continued to masturbate to porn during the above failed interventions):
A ban on any form of sexual activity was suggested. Progressive sensate focus exercises (initially non-genital and later genital) were initiated. Mr. A described an inability to experience the same degree of stimulation during penetrative sex as compared to that which he experienced during masturbation. Once the ban on masturbation was enforced, he reported an increased desire for sexual activity with his partner.
After an unspecified amount of time, the ban on masturbation to porn lead to success:
Meanwhile, Mr. A and his wife decided to go ahead with Assisted Reproductive Techniques (ART) and underwent two cycles of intrauterine insemination. During a practice session, Mr. A ejaculated for the first time, following which he has been able to ejaculate satisfactorily during a majority of the couple’s sexual interactions.
6) Pornography Induced Erectile Dysfunction Among Young Men (2019) – Abstract:
This paper explores the phenomenon of pornography induced erectile dysfunction (PIED), meaning sexual potency problems in men due to Internet pornography consumption. Empirical data from men who suffer from this condition have been collected. A combination of topical life history method (with qualitative asynchronous online narrative interviews) and personal online diaries has been employed. The data have been analyzed using theoretical interpretative analysis (according to McLuhan’s media theory), based on analytic induction. The empirical investigation indicates that there is a correlation between pornography consumption and erectile dysfunction that suggests causation. The findings are based on 11 interviews along with two video diaries and three text diaries. The men are between the ages of 16 and 52; they report that an early introduction to pornography (usually during adolescence) is followed by daily consumption until a point is reached where extreme content (involving, for example, elements of violence) is needed to maintain arousal. A critical stage is reached when sexual arousal is exclusively associated with extreme and fast-paced pornography, rendering physical intercourse bland and uninteresting. This results in an inability to maintain an erection with a real-life partner, at which point the men embark on a “re-boot” process, giving up pornography. This has helped some of the men to regain their ability to achieve and sustain an erection.
Introduction to the results section:
Having processed the data, I have noticed certain patterns and recurring themes, following a chronological narrative in all of the interviews. These are: Introduction. One is first introduced to pornography, usually before puberty. Building a habit. One begins to consume pornography regularly. Escalation. One turns to more “extreme” forms of pornography, content-wise, in order to achieve the same effects previously achieved through less “extreme” forms of pornography. Realization. One notices sexual potency problems believed to be caused by pornography use. “Re-boot” process. One tries to regulate pornography use or eliminate it completely in order to regain one’s sexual potency. The data from the interviews are presented based on the above outline.
7) Hidden in Shame: Heterosexual Men’s Experiences of Self-Perceived Problematic Pornography Use (2019) – Interviews of 15 male porn users. Several of the men reported porn addiction, escalation of use, and porn-induced sexual problems. Excerpts relevant to porn-induced sexual dysfunctions, including Michael – who significantly improve his erectile function during sexual encounters by severely limiting his porn use:
Some men talked about seeking professional help to address their problematic pornography use. Such attempts at help-seeking had not been productive for the men, and at times even exacerbated feelings of shame. Michael, a university student who used pornography primarily as a coping mechanism for study-related stress, was having issues with erectile dysfunction during sexual encounters with women and sought help from his General Practitioner Doctor (GP):
Michael: When I went to the doctor at 19 [. . .], he prescribed Viagra and said [my issue] was just performance anxiety. Sometimes it worked, and sometimes it didn’t. It was personal research and reading that showed me the issue was porn [. . .] If I go to the doctor as a young kid and he prescribes me the blue pill, then I feel like no one is really talking about it. He should be asking about my porn use, not giving me Viagra. (23, Middle-Eastern, Student)
As a result of his experience, Michael never went back to that GP and started doing his own research online. He eventually found an article discussing a man approximately his age describing a similar type of sexual dysfunction, which caused him to consider pornography as a potential contributor. After making a concerted effort to lower his pornography use, his erectile dysfunction issues began to improve. He reported that even though his total frequency of masturbation did not reduce, he only watched pornography for about half of those instances. By halving the amount of times he combined masturbation with pornography, Michael said he was able to significantly improve his erectile function during sexual encounters with women.
Phillip, like Michael, sought help for another sexual issue related to his pornography use. In his case, the problem was a noticeably reduced sex drive. When he approached his GP about his issue and its links to his pornography use, the GP reportedly had nothing to offer and instead referred him to a male fertility specialist:
Phillip: I went to a GP and he referred me to specialist who I didn’t believe was particularly helpful. They didn’t really offer me a solution and weren’t really taking me seriously. I ended up paying him for six weeks of testosterone shots, and it was $100 a shot, and it really didn’t do anything. That was their way to treat my sexual dysfunction. I just do not feel the dialogue or situation was adequate. (29, Asian, Student)
Interviewer: [To clarify a previous point you mentioned, is this the experience] that prevented you from seeking help thereafter?
Phillip: Yup.
The GPs and specialists sought by the participants seemed to offer only biomedical solutions, an approach that has been criticized within literature (Tiefer, 1996). Hence, the service and treatment these men were able to receive from their GPs was not only deemed inadequate, but also alienated them from further accessing professional help. Although biomedical responses seem to be the most popular answer for doctors (Potts, Grace, Gavey, & Vares, 2004), a more holistic and client-centered approach is needed, as the issues highlighted by men are likely psychological and possibly created by pornography use.
Lastly, men reported the impacts pornography had had on their sexual function, something that has only recently been examined within the literature. For example, Park and colleagues (2016) found that Internet pornography viewing might be associated with erectile dysfunction, decreased sexual satisfaction, and diminished sexual libido. Participants in our study reported similar sexual dysfunctions, which they attributed to pornography use. Daniel reflected on his past relationships in which he was not able to get and keep an erection. He associated his erectile dysfunction with his girlfriends’ bodies not comparing to what he had become attracted to when watching pornography:
Daniel: My previous two girlfriends, I stopped finding them arousing in a way that wouldn’t have happened to someone who was not watching porn. I had seen so many naked female bodies, that I knew the particular things that I liked and you just start forming a very clear ideal about what you want in a woman, and real women aren’t like that. And my girlfriends didn’t have perfect bodies and I think that’s fine, but I think that got in the way of finding them arousing. And that caused problems in the relationships. There are times I couldn’t sexually perform because I was not aroused. (27, Pasifika, Student)
The remaining studies are listed by date of publication:
8) The Dual Control Model – The Role Of Sexual Inhibition & Excitation In Sexual Arousal And Behavior (2007) – Newly rediscovered and very convincing. In an experiment employing video porn, 50% of the young men couldn’t become aroused or achieve erections with porn (average age was 29). The shocked researchers discovered that the men’s erectile dysfunction was,
“related to high levels of exposure to and experience with sexually explicit materials.“
The men experiencing erectile dysfunction had spent a considerable amount of time in bars and bathhouses where porn was “omnipresent,” and “continuously playing“. The researchers stated:
“Conversations with the subjects reinforced our idea that in some of them a high exposure to erotica seemed to have resulted in a lower responsivity to “vanilla sex” erotica and an increased need for novelty and variation, in some cases combined with a need for very specific types of stimuli in order to get aroused.”
9) Clinical encounters with internet pornography (2008) – Comprehensive paper, with four clinical cases, written by a psychiatrist who became aware of the negative effects internet porn was having on some of his male patients. The excerpt below describes a 31 year old man who escalated into extreme porn and developed porn-induced sexual tastes and sexual problems. This is one of the first peer-reviewed papers to depict porn use leading to tolerance, escalation, and sexual dysfunctions:
A 31-year-old male in analytic psychotherapy for mixed anxiety problems reported that he was experiencing difficulty becoming sexually aroused by his current partner. After much discussion about the woman, their relationship, possible latent conflicts or repressed emotional content (without arriving at a satisfactory explanation for his complaint), he provided the detail that he was relying on a particular fantasy to become aroused. Somewhat chagrined, he described a “scene” of an orgy involving several men and women that he had found on an Internet pornography site that had caught his fancy and become one of his favorites. Over the course of several sessions, he elaborated upon his use of Internet pornography, an activity in which he had engaged sporadically since his mid-20s. Relevant details about his use and the effects over time included clear descriptions of an increasing reliance on viewing and then recalling pornographic images in order to become sexually aroused. He also described the development of a “tolerance” to the arousing effects of any particular material after a period of time, which was followed by a search for new material with which he could achieve the prior, desired level of sexual arousal.
As we reviewed his use of pornography, it became evident that the arousal problems with his current partner coincided with use of pornography, whereas his “tolerance” to the stimulating effects of particular material occurred whether or not he was involved with a partner at the time or was simply using pornography for masturbation. His anxiety about sexual performance contributed to his reliance on viewing pornography. Unaware that the use itself had become problematic, he had interpreted his waning sexual interest in a partner to mean that she was not right for him, and had not had a relationship of greater than two months’ duration in over seven years, exchanging one partner for another just as he might change websites.
He also noted that he now could be aroused by pornographic material that he once had no interest in using. For example, he noted that five years ago he had little interest in viewing images of anal intercourse but now found such material stimulating. Similarly, material that he described as “edgier,” by which he meant “almost violent or coercive,” was something that now elicited a sexual response from him, whereas such material had been of no interest and was even off-putting. With some of these new subjects, he found himself anxious and uncomfortable even as he would become aroused.
10) Exploring the Relationship Between Erotic Disruption During the Latency Period and the Use of Sexually Explicit Material, Online Sexual Behaviors, and Sexual Dysfunctions in Young Adulthood (2009) – Study examined correlations between current porn use (sexually explicit material – SEM) and sexual dysfunctions, and porn use during “latency period” (ages 6-12) and sexual dysfunctions. The average age of participants was 22. While current porn use correlated with sexual dysfunctions, porn use during latency (ages 6-12) had an even stronger correlation with sexual dysfunctions. A few excerpts:
Findings suggested that latency erotic disruption by way of sexually explicit material (SEM) and/or child sexual abuse may be associated to adult online sexual behaviors.
Furthermore, results demonstrated that latency SEM exposure was a significant predictor of adult sexual dysfunctions.
We hypothesized that exposure to latency SEM exposure would predict adult use of SEM. Study findings supported our hypothesis, and demonstrated that latency SEM exposure was a statistically significant predictor of adult SEM use. This suggested that individuals who were exposed to SEM during latency, may continue this behavior into adulthood. Study findings also indicated that latency SEM exposure was a significant predictor of adult online sexual behaviors.
11) Use of pornography in a random sample of Norwegian heterosexual couples (2009) – Porn use was correlated with more sexual dysfunctions in the man and negative self perception in the female. The couples who did not use porn had no sexual dysfunctions. A few excerpts from the study:
In couples where only one partner used pornography, we found more problems related to arousal (male) and negative (female) self-perception.
In those couples where one partner used pornography there was a permissive erotic climate. At the same time, these couples seemed to have more dysfunctions.
The couples who did not use pornography... may be considered more traditional in relation to the theory of sexual scripts. At the same time, they did not seem to have any dysfunctions.
Couples who both reported pornography use grouped to the positive pole on the ‘‘Erotic climate’’ function and somewhat to the negative pole on the ‘‘Dysfunctions’’ function.
12) Cyber-porn dependence: voices of distress in an Italian internet self-help community (2009) – This study reports on a narrative analysis of two thousand messages written by 302 members of an Italian self-help group for cyberdependents (noallapornodipendenza). It sampled 400 messages from each year (2003–2007). Excerpts relevant to porn-induced sexual dysfunctions:
For many their condition is reminiscent of an addicted escalation with new levels of tolerance. Many of them in fact search for increasingly more explicit, bizarre and violent images, bestiality included….
Many members complain about increased impotence and lack of ejaculation, feeling in their real life like “a dead man walking” (“vivalavita” #5014). The following example concretizes their perceptions (“sul” #4411)….
Many participants stated that they usually spend hours looking at and collecting pictures and movies holding their erect penis in their hand, unable to ejaculate, waiting for the ultimate, extreme image to release the tension. For many the final ejaculation puts an end to their torture (supplizio) (“incercadiliberta” #5026)…
Problems in heterosexual relations are more than frequent. People complain they have erection problems, lack of sexual relations with their spouses, lack of interest in sexual intercourse, feeling like a person who has eaten hot, spicy food, and consequently cannot eat ordinary food. In many cases, as also reported by spouses of cyber dependents, there are indications of male orgasmic disorder with the inability to ejaculate during intercourse. This sense of desensitization in sexual relationships is well expressed in the following passage (“vivaleiene” #6019):
Last week I had an intimate relation with my girlfriend; nothing bad at all, despite the fact after the first kiss I didn’t feel any sensation. We didn’t finish the copulation because I didn’t want to.
Many participants expressed their real interest in “chatting on line” or “telematic contact” instead of physical touch, and a pervasive and unpleasant presence of pornographic flashbacks in their mind, during sleep and during sexual intercourse.
As stressed, the claim of a real sexual dysfunction is echoed by many testimonials from female partners. But also forms of collusion and contamination appear in these narratives. Here are a few of the most striking comments of these female partners…
Most of the messages sent to the Italian self help group do indicate the presence of pathology by those participants, according to the model of salience (in real life), mood modification, tolerance, withdrawal symptoms and interpersonal conflict, a diagnostic model developed by Griffiths (2004)….
13) Sexual Desire, not Hypersexuality, is Related to Neurophysiological Responses Elicited by Sexual Images (2013) – This EEG study was touted in the media as evidence against the existence of porn/sex addiction. Not so. Steele et al. 2013 actually lends support to the existence of both porn addiction and porn use down-regulating sexual desire. How so? The study reported higher EEG readings (relative to neutral pictures) when subjects were briefly exposed to pornographic photos. Studies consistently show that an elevated P300 occurs when addicts are exposed to cues (such as images) related to their addiction.
In line with the Cambridge University brain scan studies, this EEG study also reported greater cue-reactivity to porn correlating with less desire for partnered sex. To put it another way – individuals with greater brain activation to porn would rather masturbate to porn than have sex with a real person. Shockingly, study spokesperson Nicole Prause claimed that porn users merely had “high libido,” yet the results of the study say the exact opposite (subjects’ desire for partnered sex was dropping in relation to their porn use).
Together these two Steele et al. findings indicate greater brain activity to cues (porn images), yet less reactivity to natural rewards (sex with a person). That”s sensitization & desensitization, which are hallmarks of an addiction. Eight peer-reviewed papers explain the truth: Also see this extensive YBOP critique.
14) Brain Structure and Functional Connectivity Associated With Pornography Consumption: The Brain on Porn (2014) – A Max Planck study which found 3 significant addiction-related brain changes correlating with the amount of porn consumed. It also found that the more porn consumed the less reward circuit activity in response to brief exposure (.530 second) to vanilla porn. In a 2014 article lead author Simone Kühn said:
“We assume that subjects with a high porn consumption need increasing stimulation to receive the same amount of reward. That could mean that regular consumption of pornography more or less wears out your reward system. That would fit perfectly the hypothesis that their reward systems need growing stimulation.”
A more technical description of this study from a review of the literature by Kuhn & Gallinat – Neurobiological Basis of Hypersexuality (2016).
“The more hours participants reported consuming pornography, the smaller the BOLD response in left putamen in response to sexual images. Moreover, we found that more hours spent watching pornography was associated with smaller gray matter volume in the striatum, more precisely in the right caudate reaching into the ventral putamen. We speculate that the brain structural volume deficit may reflect the results of tolerance after desensitization to sexual stimuli.”
15) Neural Correlates of Sexual Cue Reactivity in Individuals with and without Compulsive Sexual Behaviours (2014) – This fMRI study by Cambridge University found sensitization in porn addicts which mirrored sensitization in drug addicts. It also found that porn addicts fit the accepted addiction model of wanting “it” more, but not liking “it” more. The researchers also reported that 60% of subjects (average age: 25) had difficulty achieving erections/arousal with real partners as a result of using porn, yet could achieve erections with porn. From the study (“CSB” is compulsive sexual behaviours):
“CSB subjects reported that as a result of excessive use of sexually explicit materials…..[they] experienced diminished libido or erectile function specifically in physical relationships with women (although not in relationship to the sexually explicit material)”
“Compared to healthy volunteers, CSB subjects had greater subjective sexual desire or wanting to explicit cues and had greater liking scores to erotic cues, thus demonstrating a dissociation between wanting and liking. CSB subjects also had greater impairments of sexual arousal and erectile difficulties in intimate relationships but not with sexually explicit materials highlighting that the enhanced desire scores were specific to the explicit cues and not generalized heightened sexual desire.”
16) Modulation of Late Positive Potentials by Sexual Images in Problem Users and Controls Inconsistent with “Porn Addiction” (2015) – A second EEG study from Nicole Prause’s team. This study compared the 2013 subjects from Steele et al., 2013 to an actual control group (yet it suffered from the same methodological flaws named above). The results: Compared to controls “individuals experiencing problems regulating their porn viewing” had lower brain responses to one-second exposure to photos of vanilla porn. The lead author claims these results “debunk porn addiction.” What legitimate scientist would claim that their lone anomalous study has debunked a well established field of study?
In reality, the findings of Prause et al. 2015 align perfectly with Kühn & Gallinat (2014), which found that more porn use correlated with less brain activation in response to pictures of vanilla porn. Prause et al. findings also align with Banca et al. 2015. Moreover, another EEG study found that greater porn use in women correlated with less brain activation to porn. Lower EEG readings mean that subjects are paying less attention to the pictures. Put simply, frequent porn users were desensitized to static images of vanilla porn. They were bored (habituated or desensitized). See this extensive YBOP critique. Nine peer-reviewed papers agree that this study actually found desensitization/habituation in frequent porn users (consistent with addiction): Peer-reviewed critiques of Prause et al., 2015
17) Adolescents and web porn: a new era of sexuality (2015) – This Italian study analyzed the effects of Internet porn on high school seniors, co-authored by urology professor Carlo Foresta, president of the Italian Society of Reproductive Pathophysiology. The most interesting finding is that 16% of those who consume porn more than once a week report abnormally low sexual desire compared with 0% in non-consumers (and 6% for those who consume less than once a week). From the study:
“21.9% define it as habitual, 10% report that it reduces sexual interest towards potential real-life partners, and the remaining, 9.1% report a kind of addiction. In addition, 19% of overall pornography consumers report an abnormal sexual response, while the percentage rose to 25.1% among regular consumers.”
18) Patient Characteristics by Type of Hypersexuality Referral: A Quantitative Chart Review of 115 Consecutive Male Cases (2015) – A study on men (average age 41.5) with hypersexuality disorders, such as paraphilias, chronic masturbation or adultery. 27 of the men were classified as “avoidant masturbators,” meaning they masturbated (typically with porn use) one or more hours per day, or more than 7 hours per week. 71% of the men who chronically masturbated to porn reported sexual functioning problems, with 33% reporting delayed ejaculation (a precursor to porn-induced ED).
What sexual dysfunction do 38% of the remaining men have? The study doesn’t say, and the authors have ignored repeated requests for details. Two primary choices for male sexual dysfunction are erectile dysfunction and low libido. It should be noted that the men were not asked about their erectile functioning without porn. This, if all their sexual activity involved masturbating to porn, and not sex with a partner, they might never realize they had porn-induced ED. (For reasons known only to her, Prause cites this paper as debunking the existence of porn-induced sexual dysfunctions.)
19) Men’s Sexual Life and Repeated Exposure to Pornography. A New Issue? (2015) – Excerpts:
Mental health specialists should take in consideration the possible effects of pornography consumption on men sexual behaviors, men sexual difficulties and other attitudes related to sexuality. In the long term pornography seems to create sexual dysfunctions, especially the individual’s inability to reach an orgasm with his partner. Someone who spends most of his sexual life masturbating while watching porn engages his brain in rewiring its natural sexual sets (Doidge, 2007) so that it will soon need visual stimulation to achieve an orgasm.
Many different symptoms of porn consumption, such as the need to involve a partner in watching porn, the difficulty in reaching orgasm, the need for porn images in order to ejaculate turn into sexual problems. These sexual behaviors may go on for months or years and it may be mentally and bodily associated with the erectile dysfunction, although it is not an organic dysfunction. Because of this confusion, which generates embarrassment, shame and denial, lots of men refuse to encounter a specialist
Pornography offers a very simple alternative to obtain pleasure without implying other factors that were involved in human’s sexuality along the history of mankind. The brain develops an alternative path for sexuality which excludes “the other real person” from the equation. Furthermore, pornography consumption in a long term makes men more prone to difficulties in obtaining an erection in a presence of their partners.
20) Masturbation and Pornography Use Among Coupled Heterosexual Men With Decreased Sexual Desire: How Many Roles of Masturbation? (2015) – Masturbating to porn was related with decreased sexual desire and low relationship intimacy. Excerpts:
Among men who masturbated frequently, 70% used pornography at least once a week. A multivariate assessment showed that sexual boredom, frequent pornography use, and low relationship intimacy significantly increased the odds of reporting frequent masturbation among coupled men with decreased sexual desire.
Among men [with decreased sexual desire] who used pornography at least once a week [in 2011], 26.1% reported that they were unable to control their pornography use. In addition, 26.7% of men reported that their use of pornography negatively affected their partnered sex and 21.1% claimed to have attempted to stop using pornography.
21) Erectile Dysfunction, Boredom, and Hypersexuality among Coupled Men from Two European Countries (2015) – Survey reported a strong correlation between erectile dysfunction and measures of hypersexuality. The study omitted correlation data between erectile functioning and pornography use, but noted a significant correlation. An excerpt:
Among Croatian and German men, hypersexuality was significantly correlated with proneness to sexual boredom and more problems with erectile function.
22) An Online Assessment of Personality, Psychological, and Sexuality Trait Variables Associated with Self-Reported Hypersexual Behavior (2015) – Survey reported a common theme found in several other studies listed here: Porn/sex addicts report greater arousabilty (cravings related to their addiction) combined with poorer sexual function (fear of experiencing erectile dysfunction).
Hypersexual” behavior represents a perceived inability to control one’s sexual behavior. To investigate hypersexual behavior, an international sample of 510 self-identified heterosexual, bisexual, and homosexual men and women completed an anonymous online self-report questionnaire battery.
Thus, the data indicated that hypersexual behavior is more common for males, and those who report being younger in age, more easily sexually excited, more sexually inhibited due to the threat of performance failure, less sexually inhibited due to the threat of performance consequences, and more impulsive, anxious, and depressed
23) Online sexual activities: An exploratory study of problematic and non-problematic usage patterns in a sample of men (2016) – This Belgian study from a leading research university found problematic Internet porn use was associated with reduced erectile function and reduced overall sexual satisfaction. Yet problematic porn users experienced greater cravings. The study appears to report escalation, as 49% of the men viewed porn that “was not previously interesting to them or that they considered disgusting.” (See studies reporting habituation/desensitization to porn and escalation of porn use) Excerpts:
“This study is the first to directly investigate the relationships between sexual dysfunctions and problematic involvement in OSAs. Results indicated that higher sexual desire, lower overall sexual satisfaction, and lower erectile function were associated with problematic OSAs (online sexual activities). These results can be linked to those of previous studies reporting a high level of arousability in association with sexual addiction symptoms (Bancroft & Vukadinovic, 2004; Laier et al., 2013; Muise et al., 2013).”
In addition, we finally have a study that asks porn users about possible escalation to new or disturbing porn genres. Guess what it found?
“Forty-nine percent mentioned at least sometimes searching for sexual content or being involved in OSAs that were not previously interesting to them or that they considered disgusting, and 61.7% reported that at least sometimes OSAs were associated with shame or guilty feelings.”
Note – This is the first study to directly investigate the relationships between sexual dysfunctions and problematic porn use. Two other studies claiming to have investigated correlations between porn use and erectile functioning cobbled together data from earlier studies in an unsuccessful attempt to debunk porn-induced ED. Both were criticized in the peer-reviewed literature: paper #1 was not an authentic study, and has been thoroughly discredited; paper #2 actually found correlations that support porn-induced sexual dysfunction. Moreover, paper 2 was only a “brief communication” that did not report important data which the authors reported at a sexology conference.
24) The effects of sexually explicit material use on romantic relationship dynamics (2016) – As with many other studies, solitary porn users report poorer relationship and sexual satisfaction. An excerpt:
More specifically, couples, where no one used, reported more relationship satisfaction than those couples that had individual users. This is consistent with the previous research (Cooper et al., 1999; Manning, 2006), demonstrating that the solitary use of SEM results in negative consequences.
Employing the Pornography Consumption Effect Scale (PCES), the study found that higher porn use was related to poorer sexual function, more sexual problems, and a “worse sex life”. An excerpt describing the correlation between the PCES “Negative Effects” on “Sex Life” questions and frequency of porn use:
There were no significant differences for the Negative Effect Dimension PCES across the frequency of sexually explicit material use; however, there were significant differences on the Sex Life subscale where High Frequency Porn Users reported greater negative effects than Low Frequency Porn Users.
25) Altered Appetitive Conditioning and Neural Connectivity in Subjects With Compulsive Sexual Behavior (2016) – “Compulsive Sexual Behaviors” (CSB) means the men were porn addicts, because CSB subjects averaged nearly 20 hours of porn use per week. The controls averaged 29 minutes per week. Interestingly, 3 of the 20 CSB subjects mentioned to interviewers that they suffered from “orgasmic-erection disorder,” while none of the control subjects reported sexual problems.
26) Associative pathways between pornography consumption and reduced sexual satisfaction (2017) – This study is found in both lists. While it links porn use to lower sexual satisfaction, it also reported that frequency of porn use was related to a preference (or need?) for porn over people to achieve sexual arousal. An excerpt:
Finally, we found that frequency of pornography consumption was also directly related to a relative preference for pornographic rather than partnered sexual excitement. Participants in the present study primarily consumed pornography for masturbation. Thus, this finding could be indicative of a masturbatory conditioning effect (Cline, 1994; Malamuth, 1981; Wright, 2011). The more frequently pornography is used as an arousal tool for masturbation, the more an individual may become conditioned to pornographic as opposed to other sources of sexual arousal.
27) “I think it has been a negative influence in many ways but at the same time I can’t stop using it”: Self-identified problematic pornography use among a sample of young Australians (2017) – Online survey of Australians, aged 15-29. Those who had ever viewed pornography (n=856) were asked in an open-ended question: ‘How has pornography influenced your life?’.
Among participants who responded to the open-ended question (n=718), problematic usage was self-identified by 88 respondents. Male participants who reported problematic usage of pornography highlighted effects in three areas: on sexual function, arousal and relationships. Responses included “I think it has been a negative influence in many ways but at the same time I can’t stop using it” (Male, Aged 18–19). Some female participants also reported problematic usage, with many of these reporting negative feelings like guilt and shame, impact on sexual desire and compulsions relating to their use of pornography. For example as one female participant suggested; “It makes me feel guilty, and I’m trying to stop. I don’t like how I feel that I need it to get myself going, it’s not healthy.” (Female, Aged 18–19)
28) Organic and psychogenic causes of sexual dysfunction in young men (2017) – A narrative review, with a section called “Role of Pornography in Delayed Ejaculation (DE)”. An excerpt from this section:
Role of Pornography in DE
Over the last decade, a large increase in the prevalence and accessibility of Internet pornography has provided increased causes of DE associated with Althof’s second and third theory. Reports from 2008 found on average 14.4% of boys were exposed to pornography before the age of 13 and 5.2% of people viewed pornography at least daily.76 A 2016 study revealed that these values had both increased to 48.7% and 13.2%, respectively.76 An earlier age of first pornographic exposure contributes to DE through its relationship with patients exhibiting CSB. Voon et al. found that young men with CSB had viewed sexually explicit material at an earlier age than their age-controlled healthy peers.75 As previously mentioned, young men with CSB can fall victim to Althof’s third theory of DE and preferentially choose masturbation over partnered sex due to a lack of arousal in relationships. An increased number of men watching pornographic material daily also contributes to DE through Althof’s third theory. In a study of 487 male college students, Sun et al. found associations between the use of pornography and a decreased self-reported enjoyment of sexually intimate behaviors with real-life partners.76 These individuals are at an elevated risk of preferentially choosing masturbation over sexual encounters, as demonstrated in a case report by Park et al. A 20-year-old enlisted male presented with difficulty achieving orgasm with his fiancée for the previous six months. A detailed sexual history revealed that the patient relied on Internet pornography and use of a sex toy described as a “fake vagina” to masturbate while deployed. Over time, he required content of an increasingly graphic or fetish nature to orgasm. He admitted that he found his fiancée attractive but preferred the feeling of his toy because he found it more stimulating that real intercourse.77 An increase in the accessibility of Internet pornography places younger men at risk of developing DE through Althof’s second theory, as demonstrated in the following case report: Bronner et al. interviewed a 35-year-old healthy man presenting with complaints of no desire to have sex with his girlfriend despite being mentally and sexually attracted to her. A detailed sexual history revealed that this scenario had happened with the past 20 women he tried to date. He reported extensive use of pornography since adolescence that initially consisted of zoophilia, bondage, sadism, and masochism, but eventually progressed to transgender sex, orgies, and violent sex. He would visualize the pornographic scenes in his imagination to function sexually with women, but that gradually stopped working.74 The gap between the patient’s pornographic fantasies and real life became too large, causing a loss of desire. According to Althof, this will present as DE in some patients.73 This recurring theme of requiring pornographic content of an increasingly graphic or fetish nature to orgasm is defined by Park et al. as hyperactivity. As a man sensitizes his sexual arousal to pornography, sex in real life no longer activates the proper neurological pathways to ejaculate (or produce sustained erections in the case of ED).77
29) Pornography increasingly damaging health and relationships says Brno’s University Hospital study (2018) – It’s in Czech. This YBOP page contains a short press release in English and a choppy Google translation of the longer press release from the hospital website. A few excerpts from the press release:
Increased use of and exposure to pornography are increasingly damaging normal relations and even the health of young men, according to a study released Monday by Brno’s University Hospital.
It said many young men were simply not prepared for normal relationships because of the myths created by the pornography they were watching. Many men turned on by pornography could not physically get stimulated in a relationship, the study added. Psychological and even medical treatment was required, the report said.
In the Sexological department of the Faculty Hospital in Brno, we also record more and more frequent cases of young men who are not able to have a normal sex life as a result of pornography, or to establish a relationship.
The fact that pornography is not merely a “diversification” of sex life but often has a negative impact on the quality of partner sexuality is evidenced by the increasing number of patients in the Sexual Section of Brno University Hospital who, due to excessive monitoring of inappropriate sexual content, are getting into health and relationship problems.
In middle age, male partners are replacing partner sex with pornography (masturbation is available anytime, faster, without psychological, physical or material investment). At the same time, sensitivity to normal (real) sexual stimuli accompanied by the risk of having sex-related dysfunctions associated only with a partner is significantly reduced by the monitoring of pornography. This is a risk of intimacy and proximity in the relationship, ie the psychological separation of partners, the need for masturbation on the Internet is gradually increasing – the risk of addiction increases and, last but not least, sexuality can change in its intensity but also in the quality of normal pornography is not enough, and these people resort to perversion (eg, sado-masochistic or zoophilous).
As a result, excessive monitoring of pornography may result in addiction, which is manifested by sexual dysfunction, disorder of relationships leading to social isolation, disrupted concentration, or neglect of work responsibilities, where only sex plays a dominant role in life.
30) Sexual Dysfunctions in the Internet Era (2018) – Excerpts:
Low sexual desire, reduced satisfaction in sexual intercourse, and erectile dysfunction (ED) are increasingly common in young population. In an Italian study from 2013, up to 25% of subjects suffering from ED were under the age of 40 [1], and in a similar study published in 2014, more than half of Canadian sexually experienced men between the age of 16 and 21 suffered from some kind of sexual disorder [2]. At the same time, prevalence of unhealthy lifestyles associated with organic ED has not changed significantly or has decreased in the last decades, suggesting that psychogenic ED is on the rise [3]. The DSM-IV-TR defines some behaviors with hedonic qualities, such as gambling, shopping, sexual behaviors, Internet use, and video game use, as “impulse control disorders not elsewhere classified”—although these are often described as behavioral addictions [4]. Recent investigation has suggested the role of behavioral addiction in sexual dysfunctions: alterations in neurobiological pathways involved in sexual response might be a consequence of repeated, supernormal stimuli of various origins.
Among behavioral addictions, problematic Internet use and online pornography consumption are often cited as possible risk factors for sexual dysfunction, often with no definite boundary between the two phenomena. Online users are attracted to Internet pornography because of its anonymity, affordability, and accessibility, and in many cases its usage could lead users through a cybersex addiction: in these cases, users are more likely to forget the “evolutionary” role of sex, finding more excitement in self-selected sexually explicit material than in intercourse.
In literature, researchers are discordant about positive and negative function of online pornography. From the negative perspective, it represents the principal cause of compulsive masturbatory behavior, cybersex addiction, and even erectile dysfunction.
31) Is Pornography Use Related to Erectile Functioning? Results From Cross-Sectional and Latent Growth Curve Analyses” (2019) – The researcher who saddled humankind with “perceived pornography addiction” and claimed it somehow “functions very differently from other addictions,” has now turned his dexterity to porn-induced ED. Even though this Joshua Grubbs-penned study found correlations between poorer sexual functioning and both porn addiction and porn use (while excluding sexually inactive men and thus many men with ED), the paper reads as if it has completely debunked porn-induced ED (PIED). This maneuver comes as no surprise to those who have followed the earlier dubious claims of Dr. Grubbs in relation to his “perceived pornography addiction” campaign. See this extensive analysis for the facts.
While the Grubbs paper consistently downplays the correlations between higher pornography use and poorer erections, correlations were reported in all 3 groups – especially for sample 3, which was the most relevant sample as it was the largest sample and averaged higher levels of porn use. Most importantly, this sample’s age range is the most likely to report PIED. Not surprisingly, sample 3 had the strongest correlation between higher levels of porn use and poorer erectile functioning (–0.37). Below are the 3 groups, with their average daily minutes of porn viewing and the correlations between erectile functioning amount of use (a negative sign means poorer erections linked to greater porn use):
- Sample 1 (147 men): average age 19.8 – Averaged 22 minutes of porn/day. (–0.18)
- Sample 2 (297 men): average age 46.5 – Averaged 13 minutes of porn/day. (–0.05)
- Sample 3 (433 men): average age 33.5 – Averaged 45 minutes of porn/day. (–0.37)
Fairly straightforward results: the sample that used the most porn (#3) had the strongest correlation between greater porn use and poorer erections, while the group that use the least (#2) had the weakest correlation between greater porn use and poorer erections. Why didn’t Grubbs emphasize this pattern in his write-up, instead of using statistical manipulations to try to make it disappear? To summarize:
- Sample #1: Average age 19.8 – Note that 19-year old porn users rarely report chronic porn-induced (especially when only using 22 minutes a day). The vast majority of porn-induced ED recovery stories YBOP has gathered are by men aged 20-40. It generally takes time to develop PIED.
- Sample #2: Average age 46.5 – They averaged only 13 minutes per day! With a standard deviation of 15.3 years, some portion of these men were fifty-something. These older men did not start out using internet porn during adolescence (making them less vulnerable to conditioning their sexual arousal solely to internet porn). Indeed, just as Grubbs found, the sexual health of slightly older men has always been better and more resilient over all, than users who began using digital porn during adolescence (such as those with an average age of 33 in sample 3).
- Sample #3: Average age 33.5 – As already mentioned, sample 3 was the largest sample and averaged higher levels of porn use. Most importantly, this age range is the most likely to report PIED. Not surprisingly, sample 3 had the strongest correlation between higher levels of porn use and poorer erectile functioning (–0.37).
Grubbs also correlated porn addiction scores with erectile functioning. The results reveal that even in subjects with relatively healthy erectile functioning, porn addiction was significantly related to poorer erections (–0.20 to –0.33). As before, the strongest correlation between porn addiction and poorer erections (–0.33) occurred in Grubbs’s largest sample, and the sample of an average age most likely to report porn-induced ED: sample 3, average age: 33.5 (433 subjects).
Wait a minute you ask, how dare I say significantly related? Doesn’t the Grubbs study confidently declare that the relationship was only “small to moderate,” meaning it’s no big deal? As we explored in the critique, Grubbs’s use of descriptors varies remarkably, depending upon which Grubbs study you read. If the Grubbs study is about porn use causing ED, then the above numbers represent a meager correlation, tossed aside in his spin-laden write-up.
However, if it’s Grubbs’s most famous study (“Transgression as Addiction: Religiosity and Moral Disapproval as Predictors of Perceived Addiction to Pornography“), where he proclaimed that being religious was the real cause of “porn addiction,” then numbers smaller than these constitute a “robust relationship.” In fact, Grubbs’s “robust” correlation between religiosity and “perceived pornography addiction” was only 0.30! Yet he audaciously used it to usher in a completely new, and questionable, model of porn addiction. The tables, correlations and details referred to here are found in this section of a longer YBOP analysis.
32) Survey of Sexual Function and Pornography (2019) – In this study, researchers looked for a link between ED and indices of pornography addiction using a “craving” questionnaire. While no such link turned up (perhaps because users don’t accurately assess their degree of “craving” until they attempt to quit using), some other interesting correlations appeared in their results. Excerpts:
Rates of erectile dysfunction were lowest in those [men] preferring partnered sex without pornography (22.3%) and increased significantly when pornography was preferred over partnered sex (78%).
…Pornography and sexual dysfunction are common among young people.
…Those [men] who used on an almost daily basis or more had ED rates of 44% (12/27) compared to 22% (47/213) for those more “casual” users (≤5x/week), reaching significance on univariate analysis (p=0.017). It may be that volume does play a role to some extent.
…The proposed pathophysiology of PIED seems plausible and is based on a variety of researchers work and not a small collection of researchers that might be swayed by an ethical bias. Also supporting the “causation” side of the argument are reports of men regaining normal sexual function after discontinuation of excessive pornography use.
…Only prospective studies will be able to definitively solve the question of causation or association, including interventional studies evaluating the success of abstention in treating ED in heavy pornography users. Additional populations that warrant special consideration include adolescents. There has been concern raised that early exposure to graphic sexual material may affect normal development. The rate of teenagers being exposed to pornography before the age of 13 has gone up three fold over the last decade, and now hovers around 50%.
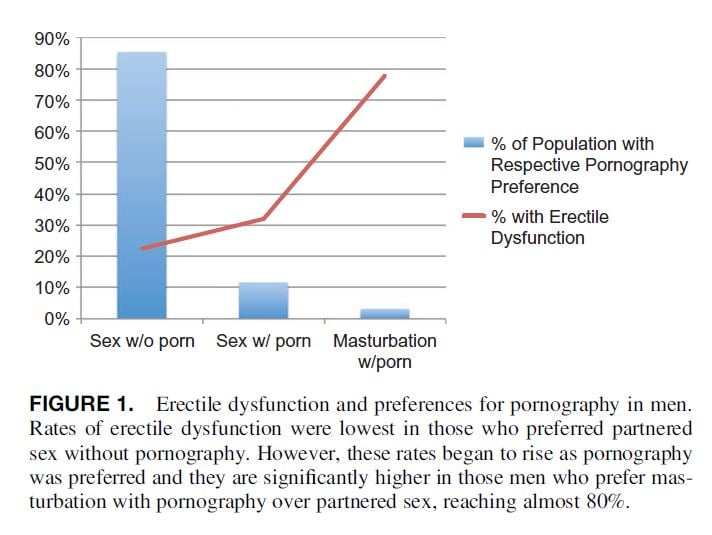
The above study was presented at the American Urological Association’s 2017 meeting. A few excerpts from this article about it – Study sees link between porn and sexual dysfunction (2017):
Young men who prefer pornography to real-world sexual encounters might find themselves caught in a trap, unable to perform sexually with other people when the opportunity presents itself, a new study reports. Porn-addicted men are more likely to suffer from erectile dysfunction and are less likely to be satisfied with sexual intercourse, according to survey findings presented Friday at the American Urological Association’s annual meeting, in Boston.
“The rates of organic causes of erectile dysfunction in this age cohort are extremely low, so the increase in erectile dysfunction that we have seen over time for this group needs to be explained,” Christman said. “We believe that pornography use may be one piece to that puzzle”.
33) Sexual Dysfunction in the New Father: Sexual Intimacy Issues (2018) – This chapter from a new medical textbook entitled Paternal Postnatal Psychiatric Illnesses addresses porn’s impact on the sexual function of a new father, citing a paper co-authored by this website’s host, “Is Internet Pornography Causing Sexual Dysfunctions? A Review with Clinical Reports.” This page contains screenshots of relevant excerpts from the chapter.
34) Prevalence, Patterns and Self-Perceived Effects of Pornography Consumption in Polish University Students: A Cross-Sectional Study (2019) Large study (n = 6463) on male & female college students (median age 22) reports relatively high levels of porn addiction (15%), escalation of porn use (tolerance), withdrawal symptoms, and porn-related sexual & relationship problems. Relevant excerpts:
The most common self-perceived adverse effects of pornography use included: the need for longer stimulation (12.0%) and more sexual stimuli (17.6%) to reach orgasm, and a decrease in sexual satisfaction (24.5%)…
The present study also suggests that earlier exposure may be associated with potential desensitization to sexual stimuli as indicated by a need for longer stimulation and more sexual stimuli required to reach orgasm when consuming explicit material, and overall decrease in sexual satisfaction…
Various changes of pattern of pornography use occurring in the course of the exposure period were reported: switching to a novel genre of explicit material (46.0%), use of materials that do not match sexual orientation (60.9%) and need to use more extreme (violent) material (32.0%)…
35) Sexual and reproductive health and rights in Sweden 2017 (2019) – A 2017 survey by The Swedish Public Health Authority contains a section discussing their findings on pornography. relevant here, greater pornography use was related to poorer sexual health and decreased sexual dissatisfaction. Excerpts:
Forty-one percent of men aged 16 to 29 are frequent users of pornography, i.e. they consume pornography on a daily basis or almost on a daily basis. The corresponding percent among women is 3 percent. Our results also show an association between frequent pornography consumption and poorer sexual health, and an association with transactional sex, too high expectations of one’s sexual performance, and dissatisfaction with one’s sex life. Almost half of the population state that their pornography consumption does not affect their sex life, while a third do not know if it affects it or not. A small percentage of both women and men say their pornography use has a negative effect on their sex life. It was more common among men with higher education to regularly use pornography compared to men with lower education.
There is a need for more knowledge on the link between pornography consumption and health. An important preventive piece is to discuss the negative consequences of pornography with boys and young men, and school is a natural place to do this.
36) Internet Pornography: Addiction or Sexual Dysfunction? (2019) – Link to PDF of the chapter in Introduction to Psychosexual Medicine (2019) – White, Catherine. “Internet Pornography: Addiction or Sexual Dysfunction. Introduction to Psychosexual Medicine?” (2019)
37) Abstinence or Acceptance? A Case Series of Men’s Experiences With an Intervention Addressing Self-Perceived Problematic Pornography Use (2019) – The paper reports on six cases of men with porn addiction as they underwent a mindfulness-based intervention program (meditation, daily logs & weekly check-ins). All 6 subjects seemed to benefit from meditation. Relevant to this list of studies, 2 of 6 reported porn-induced ED. A few report escalation of use (habituation). One describes withdrawal symptoms. Excerpts from the cases reporting PIED:
Pedro (age 35):
Pedro self-reported as being a virgin. Pedro talked about the feelings of shame he experienced with his past attempts at sexual intimacy with women. His most recent potential sexual encounter ended when his fear and anxiety prevented him from getting an erection. He attributed his sexual dysfunction to pornography use…
Pedro reported a significant decrease in pornography viewing by the end of the study and an overall improvement in mood and mental health symptoms. Despite increasing the dosage of one of his anti-anxiety medications during the study due work stress, he said he would continue meditating because of the self-reported benefits of calmness, focus, and relaxation he experienced after each session.
Pablo (age 29):
Pablo felt he had little to no control over his pornography use. Pablo spent several hours each day ruminating on pornography, either while actively engaged in watching pornographic content or by thinking about watching pornography at the next possible opportunity when he was busy doing something else. Pablo went to a doctor with concerns about sexual dysfunctions he was experiencing, and though he disclosed concerns about his pornography use to his doctor, Pablo was instead referred to a male fertility specialist where he was given shots of testosterone. Pablo reported the testosterone intervention as having no benefit or usefulness to his sexual dysfunction, and the negative experience prevented him from reaching out for any further help with regards to his pornography use. The pre-study interview was the first time Pablo was able to converse openly with anybody regarding his pornography use…
38) Lecture describing upcoming studies – by Urology professor Carlo Foresta, president of the Italian Society of Reproductive Pathophysiology – The lecture contains the results of longitudinal and cross-sectional studies. One study involved a survey of high school teens (pages 52-53). The study reported that sexual dysfunction doubled between 2005 and 2013, with low sexual desire increasing 600%.
- The percentage of teens that experienced alterations of their sexuality: 2004/05: 7.2%, 2012/13: 14.5%
- The percentage of teens with low sexual desire: 2004/05: 1.7%, 2012/13: 10.3% (that’s a 600% increase in 8 years)
Foresta also describes his upcoming study, “Sexuality media and new forms of sexual pathology sample 125 young males, 19-25 years” (Italian name – “Sessualità mediatica e nuove forme di patologia sessuale Campione 125 giovani maschi“). The results from the study (pages 77-78), which used the International Index of Erectile Function Questionnaire, found that regular porn users scored 50% lower on sexual desire domain and 30% lower of the erectile functioning domain.
39) (not peer-reviewed) Here’s an article about an extensive analysis of comments and questions posted on MedHelp concerning erectile dysfunction. What’s shocking is that 58% of the men asking for help were 24 or younger. Many suspected that internet porn could be involved as described in the results from the study –
The most common phrase is “erectile dysfunction” – which is mentioned more than three times as often as any other phrase – followed by “internet porn,” “performance anxiety,” and “watching porn.”
Clearly, porn is a frequently discussed subject: “I have been viewing internet pornography frequently (4 to 5 times a week) for the past 6 years,” one man writes. “I am in my mid-20s and have had a problem getting and maintaining an erection with sexual partners since my late teens when I first started looking at internet porn.”
Article about the latest spin campaign: Sexologists Deny Porn-induced ED by Claiming Masturbation Is the Problem (2016)
DAVID LEY: However, Dr. Zimbardo fails to acknowledge or consider the tremendous social changes which occurred with the invention of erectile performance medications, and which dramatically increased willingness to disclose erectile dysfunction, by reducing the shame associated with it.
RESPONSE: Studies assessing young male sexuality since 2010 report historic levels of sexual dysfunctions, and startling rates of a new scourge: low libido. Documented in this lay article and in this peer-reviewed paper involving 7 US Navy doctors – Is Internet Pornography Causing Sexual Dysfunctions? A Review with Clinical Reports (2016)
Ley cited nothing as, once again, there is no empirical support for his claim that the introduction of Viagra (1997) led to men finally tell the truth in studies on sexual dysfunction (13 years later). These are not the rates of men visiting their doctors to request ED medication. The ED rates cited refer only to peer-reviewed studies (usually anonymous) on population wide rates of sexual dysfunction. To put it another way, the ‘Viagra hypothesis’ is claiming that in every single study published between 1948 and 2010, in countries all over the world, the young male participants consistently lied about their erectile functioning. Then, all of a sudden, in 2010 all the young men (and only the young men) began to tell the truth about their ED problems. This is absurd. Ley’s claim is like saying that the introduction of aspirin led to anonymous studies reporting a 1000% increase in headaches among only one age group. A few more points that refute the “Viagra causes ED” claim:
1) The claim about “willingness to disclose” doesn’t apply here. The ED and low libido rates are not rates for men visiting their doctor for erectile dysfunction. Instead, the ED and low libido rates come from studies mostly employing anonymous standardized questionnaires where men rate the quality of their erections and arousal during sex. That has not changed because Viagra was introduced.
2) The exponential rise in ED and low libido rates occurred only in men under 40. This alone refutes Ley’s claim.
3) In this same time period there was a concomitant increase in low sexual desire (and evidence of increases in difficulty orgasming too). The largest US study from 1992 reported 5% of men under 40 had low sexual desire.
- A 2014 Canadian study reported low sexual desire in 24% of 16-21 year olds!
- A 2014 survey of Croatian men 40 and under reported low sexual desire rates of 37%.
- Again, this aligns with a 2015 study on Italian high school seniors (18-19), which found that 16% of those who use porn more than once per week reported abnormally low sexual desire. Non-porn users reported 0% low sexual desire (as one would expect in 18-year olds).
4) These days, ED rates are often higher for young men than for old men (who obviously used less internet porn growing up). The 2014 Canadian study reported that 53.5% of males aged 16-21 have symptoms indicative of a sexual problem. Erectile dysfunction was the most common (27%), followed by low sexual desire (24%), and problems with orgasm (11%).
- Reality check: these rates are higher than those reported for 50-60 year olds in the large 1992 study on men 18-60!
5) Two studies published AFTER Viagra was introduced report higher ED rates in young men. If Viagra ads caused ED in men, wouldn’t we see far higher rates in older men? These were studies of the same European countries using the same questionnaires (GSSAB). Instead rates in young men are abnormally high now.
- The 2001-2002 ED rates for men 40-80 were about 13% in Europe.
- By 2011, ED rates in young Europeans, 18-40, ranged from 14-28%.
6) Common sense: There’s absolutely no evidence to suggest that a young man today would be any less embarrassed or ashamed when experiencing erectile dysfunction than a young man was in 1995 (once again, shame is irrelevant as all data came from studies using anonymous questionnaires).
DAVID LEY: Indeed, multiple peer-reviewed articles have now been published which found no evidence for PIED, but instead, found the opposite effect, that porn use and concomitant masturbation, is likely to result in delayed orgasm.
RESPONSE TO FIRST PART: “multiple peer-reviewed articles have now been published which found no evidence for PIED”
First, there’s only one way to confirm whether erectile dysfunction is porn-induced (PIED) or not: Eliminate porn use for a extended period of time and see if the sufferer regains normal erectile functioning. Three studies have done this, thus proving the existence of porn-induced sexual dysfunctions. See this list of 28 studies linking porn use/sex addiction to sexual problems (the first 5 demonstrate causation as participants eliminated porn use and healed chronic sexual dysfunctions).
The “multiple articles” that Ley could be referring to are really only two papers that claimed to have found little relationship between the amount of porn use and erectile dysfunction. The first paper, Prause & Pfaus 2015, has been so roundly criticized for missing data, unsupported claims, poor methodology, and statements that are in direct opposition of its data, that it is, in effect, discredited. It was formally critiqued in an academic journal by a researcher and reproductive medicine doctor. This lay critique exposes even more holes in the paper.
A second paper (Landripet & Stulhofer) found extraordinarily high rates of low libido and ED in men under 40 (it wasn’t a full study, but a “brief communication”). Contrary to Ley’s claims, the study actually found a few correlations between ED and porn use. The abstract doesn’t mention a pretty important correlation: Only 40% of the Portuguese men used porn “frequently,” while the 60% of the Norwegians used porn “frequently.” The Portuguese men had far less sexual dysfunction than the Norwegians.
Elsewhere, the authors acknowledge a statistically significant association between more frequent porn use and ED, but claim the effect size was small. However, this claim may be misleading according to an MD who is a skilled statistician and has authored many studies:
Analyzed a different way (Chi Squared), … moderate use (vs. infrequent use) increased the odds (the likelihood) of having ED by about 50% in this Croatian population. That sounds meaningful to me, although it is curious that the finding was only identified among Croats.
Here’s the sneaky part that says a lot about the two authors: Landripet & Stulhofer’s “brief communication” omitted three significant correlations they presented to a European conference (excerpts from their abstract):
Reporting a preference for specific pornographic genres were significantly associated with erectile (but not ejaculatory or desire-related) male sexual dysfunction.
Increased pornography use was slightly but significantly associated with decreased interest for partnered sex and more prevalent sexual dysfunction among women
The authors blow this finding off and ignore it in reaching their conclusions, as they also ignore Danish porn researcher Gert Martin Hald’s formal commentary about the study, in which he says:
However, in pornography research, the interpretation of “size” may depend as much on the nature of the outcome studied as the magnitude of the relationship found. Accordingly, if the outcome is to be considered “sufficiently adverse” (e.g., sexual aggressive behaviors), even small effect sizes may carry considerable social and practical significance [2].
Gert Martin Hald’s editorial comments emphasize the need to assess more variables (mediators, moderators) than just frequency per week in the last 12 months:
Third, the study does not address possible moderators or mediators of the relationships studied nor is it able to determine causality. Increasingly, in research on pornography, attention is given to factors that may influence the magnitude or direction of the relationships studied (i.e., moderators) as well as the pathways through which such influence may come about (i.e., mediators). Future studies on pornography consumption and sexual difficulties may also benefit from an inclusion of such focuses.
In other words, using only a single limited variable such as “hours of use in the last month” may not reveal anything. It’s already established in studies on both internet porn addiction (1, 2, 3) and internet video-gaming addiction, that symptoms do not correlate with “hours of use.” Instead of just current hours of use, a combination of variables appears to correlate best with porn-induced ED. These may include:
- Ratio of masturbation to porn versus masturbation without porn
- Ratio of sexual activity with a person versus masturbation to porn
- Gaps in partnered sex (where one relies only on porn)
- Virgin or not
- Total hours of use
- Years of use
- Age started using porn
- Escalation to new genres
- Development of porn-induced fetishes (from escalating to new genres of porn)
- Level of novelty per session (i.e. compilation videos, multiple tabs)
- Addiction-related brain changes or not
- Presence of hypersexuality/porn addiction
The better way to research the phenomenon of porn-induced sexual dysfunctions, is to remove the variable of internet porn use and observe the outcome. Such research reveals causation instead of correlations open to interpretation. My site has documented a few thousand men who removed internet porn and recovered from chronic sexual dysfunctions.
SUMMARY: Only one valid study has attempted to correlate the amount of porn use with ED. Contrary to Ley’s claim, this study reports at least one meaningful correlation between ED and porn use. Offsetting this single “brief communication,” we have 25 studies reporting relationships between porn use in young men and ED, anorgasmia, low sexual desire, delayed ejaculation and lower brain activation to sexual images.
DAVID LEY: “Indeed, multiple peer-reviewed articles have now been published which found no evidence for PIED, but instead, found the opposite effect, that porn use and concomitant masturbation, is likely to result in delayed orgasm.”
RESPONSE TO SECOND PART: “but instead, found the opposite effect, that porn use and concomitant masturbation, is likely to result in delayed orgasm.”
How bizarre. Ley appears to be claiming that delayed orgasm is “the opposite” of erectile dysfunction. Hats off to Ley. This has to be the most over-the-top bits of spin he’s ever written. Ley appears to be spinning the results of this 2015 study on men with hypersexuality disorders – “Patient Characteristics by Type of Hypersexuality Referral: A Quantitative Chart Review of 115 Consecutive Male Cases”.
The study classified 27 men as “avoidant masturbators,” meaning they masturbated to porn one or more hours per day or more than 7 hours per week. 71% of the compulsive porn users reported sexual functioning problems, with 33% reporting delayed ejaculation.
What sexual dysfunction do 38% of the remaining men have? The study doesn’t say, and the authors have publicly refused to give details. The two other primary choices for male sexual dysfunction are ED and low libido. You do the math.
In reality, porn-induced delayed ejaculation is often a precursor to porn-induced erectile dysfunction. Like ED, delayed ejaculation is one of the primary reasons men choose to abstain from porn in search of recovery. This page contains many stories by men who recovered from porn-induced delayed ejaculation. Delayed ejaculation arises from the same brain changes that eventually lead to full blown PIED (i.e. desensitization/habituation and conditioning one’s sexual arousal to everything associated with internet porn use instead of to real partners).
SUMMARY: Ley is trying to spin a 71% rate of sexual dysfunction in compulsive porn users into evidence that porn use is really beneficial! That’s Ley as his best.
DAVID LEY: Numerous research studies in the past year from authors such as Joshua Grubbs of Case Western and Alexander Stulhofer of Croatia, have consistently confirmed the role of morality and religiosity in the backgrounds of those who identify as sex or porn addicts. In other words, both of these researchers have demonstrated that sex/porn addicts are not in fact watching more porn or having more sex than anyone else – they just feel worse and more conflicted about the sex they are having.
RESPONSE: Numerous? Since there are no citations let’s consider the two studies mentioned: In the case of Grubbs and Stulhofer how have the researchers distinguished between shame related to sex/porn and shame from the inability to control use despite negative consequences? This is left unexplained. (In other words, they haven’t.)
As for Stulhofer paper (Is High Sexual Desire a Facet of Male Hypersexuality? Results from an Online Study) It’s conclusion says:
Compared to the rest of the sample, men in the hypersexuality group had significantly higher odds of being single, not exclusively heterosexual, religious, depressed, prone to sexual boredom, experiencing substance abuse consequences, holding negative attitudes toward pornography use, and evaluating one’s sexual morality more negatively. In contrast, the high sexual desire group differed from controls only in reporting more positive attitudes toward pornography use.
First, Stulhofer reported very little overlap between the hypersexuality group (sex/porn addicts) and the high libido group. As explained above, this refutes Ley’s claim that “hypersexuals” simply have high sexual desire.
Second, the addicts held negative attitudes towards pornography use. Is it really so odd for an addict to feel bad about being unable to control use despite the negative consequences? Wouldn’t we expect an out-of-control alcoholic to have negative feelings towards drinking alcohol? What does the phrase “evaluating one’s sexual morality” mean when it is applied to out-of-control porn use that is impacting one’s life negatively? It could be as simple as, “Addicts experience negative feelings towards their addiction.”
As for Grubbs et al‘s results, might they be explained, in part, by the fact that religious people are generally better informed (or, in some cases overly informed) about the risks of internet porn use, so they “connect the dots” more quickly and in higher percentages when asked about their addiction? Religious people are probably also more inclined to try stopping, and therefore more likely to experience distressing withdrawal symptoms or recognize their inability to control their (perhaps) infrequent use. Withdrawal symptoms are anxiety-producing in themselves. In contrast, the non-religious simply don’t think to experiment with stopping porn so they may not experience severe cravings and withdrawal symptoms unless they slam into a wall o’ hurt and try quitting.
If religion were the key factor in a “belief in porn addiction,” one would expect the majority of those on the recovery forums to be religious. That is not what we see. The most popular English-speaking porn-recovery forum we know of, r/nofap, polled their members (back in 2012). 60+% of their members were non-religious (23% Christian). Shortly after that poll, a “Christian nofap” was founded, which means that the percentage of religious on r/nofap is even lower now. In a later member survey, only 11% were quitting for religious reasons. Since that first poll, the number of members on r/nofap has exploded. It’s 170K+ members now, and overwhelming non-religious.
Grubbs needs better methodology – methodology that does not conflate shame arising from “being unable to quit an addiction that is producing negative effects” with shame arising from porn’s content. Two quite different phenomena.
Is it Ethical for a Psychologist to Consistently Attack a Self-Help Group?
Ley suggests that NoFap, a porn-recovery forum, is somehow dangerous. In this piece he continues his ongoing defamatory attacks on the NoFap community. If he disagrees with the scientific findings on internet porn users’ brains (which support the efforts on NoFap), he should take it up with the researchers themselves, not take it out on a self-help community. This is like attacking cancer patients because one disagrees with oncology protocols.
Not only is it disturbing that Ley attacks people endeavoring to recover from the effects of over-consuming internet porn, it may be a violation of various principles of the American Psychological Association. The APA has 5 guiding principles for all psychologists and Ley’s chronic disparaging of NoFap appears to violate all 5:
Principle A: Beneficence 4.05 and Nonmaleficence (in part)
… In their professional actions, psychologists seek to safeguard the welfare and rights of those with whom they interact professionally and other affected persons… …. Because psychologists’ scientific and professional judgments and actions may affect the lives of others, they are alert to and guard against personal, financial, social, organizational or political factors that might lead to misuse of their influence…
Principle B: Fidelity and Responsibility (in part)
Psychologists … are aware of their professional and scientific responsibilities to society and to the specific communities in which they work. Psychologists uphold professional standards of conduct, clarify their professional roles and obligations, accept appropriate responsibility for their behavior and seek to manage conflicts of interest that could lead to exploitation or harm. …
Principle C: Integrity (in part)
Psychologists seek to promote accuracy, honesty and truthfulness in the science, teaching and practice of psychology. In these activities psychologists do not steal, cheat or engage in fraud, subterfuge or intentional misrepresentation of fact.
Principle D: Respect for People’s Rights (in part)
Psychologists exercise reasonable judgment and take precautions to ensure that their potential biases, the boundaries of their competence and the limitations of their expertise do not lead to or condone unjust practices.
Principle E: Dignity (in part)
Psychologists respect the dignity and worth of all people, and the rights of individuals to privacy, confidentiality, and self-determination.
David Ley financial conflicts of interest (COI)
COI #1: In a blatant financial conflict of interest, David Ley is being compensated by porn industry giant X-hamster to promote their websites and to convince users that porn addiction and sex addiction are myths! Specifically, David Ley and the newly formed Sexual Health Alliance (SHA) have partnered with a X-Hamster website (Strip-Chat). See “Stripchat aligns with Sexual Health Alliance to stroke your anxious porn-centric brain“:

The fledgling Sexual health Alliance (SHA) advisory board includes David Ley and two other RealYourBrainOnPorn.com “experts” (Justin Lehmiller & Chris Donahue). RealYBOP is a group of openly pro-porn, self-proclaimed “experts” headed by Nicole Prause. This group is currently engaged in illegal trademark infringement and squatting directed toward the legitimate YBOP. Put simply, those trying to silence YBOP are also being paid by the porn industry to promote its/their businesses, and assure users that porn and cam sites cause no problems (note: Nicole Prause has close, public ties to the porn industry as thoroughly documented on this page).
In this article, Ley dismisses his compensated promotion of the porn industry:
Granted, sexual health professionals partnering directly with commercial porn platforms face some potential downsides, particularly for those who’d like to present themselves as completely unbiased. “I fully anticipate [anti-porn advocates] to all scream, ‘Oh, look, see, David Ley is working for porn,’” says Ley, whose name is routinely mentioned with disdain in anti-masturbation communities like NoFap.
But even if his work with Stripchat will undoubtedly provide fodder to anyone eager to write him off as biased or in the pocket of the porn lobby, for Ley, that tradeoff is worth it. “If we want to help [anxious porn consumers], we have to go to them,” he says. “And this is how we do that.”
Biased? Ley reminds us of the infamous tobacco doctors, and the Sexual health Alliance, the Tobacco Institute.
COI #2 David Ley is being paid to debunk porn and sex addiction. At the end of this Psychology Today blog post Ley states:
“Disclosure: David Ley has provided testimony in legal cases involving claims of sex addiction.”
In 2019 David Ley’s new website offered his well-compensated “debunking” services:
David J. Ley, Ph.D., is a clinical psychologist and AASECT-certified supervisor of sex therapy, based in Albuquerque, NM. He has provided expert witness and forensic testimony in a number of cases around the United States. Dr. Ley is regarded as an expert in debunking claims of sexual addiction, and has been certified as an expert witness on this topic. He has testified in state and federal courts.
Contact him to obtain his fee schedule and arrange an appointment to discuss your interest.
COI #3: Ley makes money selling two books that deny sex and porn addiction (“The Myth of Sex Addiction,” 2012 and “Ethical Porn for Dicks,” 2016). Pornhub (which is owned by porn giant MindGeek) is one of the five back-cover endorsements listed for Ley’s 2016 book about porn:
Note: PornHub was the second Twitter account to retweet RealYBOP’s initial tweet announcing its “expert” website, suggesting a coordinated effort between PornHub and the RealYBOP experts. Wow!
COI #4: Finally, David Ley makes money via CEU seminars, where he promotes the addiction-deniers’ ideology set forth in his two books (which recklessly ignores (which recklessly ignores hundreds of studies and the significance of the new Compulsive Sexual Behavior Disorder diagnosis in the World Health Organization’s diagnostic manual). Ley is compensated for his many talks featuring his biased views of porn. In this 2019 presentation Ley appears to support and promote adolescent porn use: Developing Positive Sexuality and Responsible Pornography Use in Adolescents.