Introduction
This critique has two parts: Part 1 exposes how Nicole Prause, Marty Klein and Taylor Kohut completely misrepresent their solitary bit of “evidence” to support the article’s core falsehood – that “compulsive pornography viewing” was excluded from the new ICD-11 “Compulsive Sexual Behavior Disorder” diagnosis. Part 2 exposes the startling omissions, false claims, research misrepresentations, and cherry-picked data littering the Prause/Klein/Kohut article. (Note: Most of the article’s cherry-picked data and misrepresentations are recycled from this 2016 Prause “Letter to the editor” that YBOP thoroughly dismantled 2 years ago: Critique of: Letter to the editor “Prause et al. (2015) the latest falsification of addiction predictions”, 2016.)
Who are the authors of this article?
Before reviewing the details below, it would be well to consider the mouthpieces of the brazen serving of propaganda in Slate. Its authors are not impartial observers. Their pro-porn agenda is plain.
Nicole Prause is a former academic with a long history of harassing and defaming authors, researchers, therapists, reporters, men in recovery, Journal editors, multiple organizations, and others who dare to report evidence of harms from internet porn use. She appears to be quite cozy with the pornography industry, as can be seen from this image of her (far right) on the red carpet of the X-Rated Critics Organization (XRCO) awards ceremony. (According to Wikipedia the XRCO Awards are given by the American X-Rated Critics Organization annually to people working in adult entertainment and it is the only adult industry awards show reserved exclusively for industry members.[1]).
It also appears that Prause may have obtained porn performers as subjects through another porn industry interest group, the Free Speech Coalition. The FSC subjects were allegedly used in her hired-gun study on the heavily tainted and very commercial “Orgasmic Meditation” scheme (which is now being investigated by the FBI). Prause has also made unsupported claims about the results of her studies and her study’s methodologies. For much more documentation, see: Is Nicole Prause Influenced by the Porn Industry?.
Marty Klein once boasted his very own webpage on the AVN’s Hall of Fame in recognition of his pro-porn advocacy serving the porn industry’s interests (since removed).
Taylor Kohut is a Canadian researcher who publishes biased, carefully contrived research such as: “Is Pornography Really about ‘Making Hate to Women’?” which would have gullible readers believe that porn users hold more egalitarian attitudes toward women (they don’t), and “Perceived Effects of Pornography on the Couple Relationship,” which attempts to counter the over 75 studies showing that porn use has negative effects on relationships. (Here’s a Vimeo presentation critiquing highly questionable Kohut and Prause studies.) Kohut’s new website and his attempt at fundraising suggest that he just may have an agenda. Kohut’s bias was clearly revealed in a brief written for the Standing Committee on Health Regarding Motion M-47 (Canada). In the brief, as in the Slate article, Kohut and his coauthors were guilty of cherry-picking a few outlying studies while misrepresenting the current state of the research on porn’s effects.
- Update (April, 2019): In an attempt to silence YBOP’s criticism, a handful of authors formed a group to steal YBOP’s trademark (headed by Nicole Prause and including Marty Klein & Taylor Kohut). See this page for details: Aggressive Trademark Infringement Waged by Porn Addiction Deniers (www.realyourbrainonporn.com). If you are looking for an analysis of a study that you cannot in the following critique check this page: Porn Science Deniers Alliance (AKA: “RealYourBrainOnPorn.com” and “PornographyResearch.com”). It examines the trademark infringers’ “research page,” including its cherry-picked outlier studies, bias, egregious omission, and deception.
- Update (Summer, 2019): On May 8, 2019 Donald Hilton, MD filed a defamation per se lawsuit against Nicole Prause & Liberos LLC. On July 24, 2019 Donald Hilton amended his defamation complaint to highlight (1) a malicious Texas Board of Medical Examiners complaint, (2) false accusations that Dr. Hilton had falsified his credentials, and (3) affidavits from 9 other Prause victims of similar harassment & defamation (John Adler, MD, Gary Wilson, Alexander Rhodes, Staci Sprout, LICSW, Linda Hatch, PhD, Bradley Green, PhD, Stefanie Carnes, PhD, Geoff Goodman, PhD, Laila Haddad.)
- Update (October, 2019): On October 23, 2019 Alexander Rhodes (founder of reddit/nofap and NoFap.com) filed a defamation lawsuit against Nicole R Prause and Liberos LLC. See the court docket here. See this page for three primary court documents filed by Rhodes: NoFap founder Alexander Rhodes defamation lawsuit against Nicole Prause / Liberos.
- Update (November, 2019): Finally, some accurate media coverage: “Alex Rhodes of Porn Addiction Support Group ‘NoFap’ Sues Obsessed Pro-Porn Sexologist for Defamation” by Megan Fox of PJ Media and “Porn wars get personal in No Nut November”, by Diana Davison of The Post Millennial. Davison also produced this 6-minute video about Prause’s egregious behaviors: “Is Porn Addictive?”.
PART 1: Debunking claim ICD-11 excluded “pornography viewing” from “Compulsive Sexual Behavior Disorder” diagnosis
The deniers of porn addiction are agitated because the latest version of the World Health Organization’s medical diagnostic manual, The International Classification of Diseases (ICD-11), contains a new diagnosis suitable for diagnosing what is commonly referred to as ‘porn addiction’ or ‘sex addiction’. It’s called “Compulsive Sexual Behavior Disorder” (CSBD). Nonetheless, in a bizarre “We lost, but we won” propaganda campaign, the deniers have been pulling out all the stops to spin this new diagnosis as a rejection of both “sex addiction” and “porn addiction.”
Not satisfied with the false narrative claiming a “rejection of addiction,” veteran porn-addiction deniers Nicole Prause, Marty Klein and Taylor Kohut have taken their propaganda to new levels in this July 30, 2018 Slate article: “Why Are We Still So Worried About Watching Porn?” Without supplying any evidence beyond mere opinions, the Prause/Klein/Kohut triumvirate asserts that WHO has officially excluded pornography viewing from the “Compulsive Sexual Behavior Disorder” diagnosis:
With no support, and zero logic, Prause/Klein/Kohut would have us believe that the most common compulsive sexual behavior – compulsive pornography use – has been axed from the WHO’s new diagnostic manual edition (the ICD-11). The hollowness of the authors’ campaign is apparent for many reasons, some of the most obvious of which are:
- It is self-evident that the language itself of the CSBD diagnosis applies to those struggling with compulsive pornography use. (See below.)
- CSBD does not describe (or exclude) any particular sexual activity.
- Multiple studies show that at least 80% of people with compulsive sexual behaviour (hypersexuality) report compulsive internet pornography use.
- Most of the recent 50 neuroscience-based studies (on which the WHO relied in its decision to include CSBD) have been done on internet pornography viewers – so it is silly to suggest that the WHO intended to exclude pornography viewing but forgot to specify it.
Before we get to a detailed evaluation of the deniers’ remarks, let’s be clear: There is neither proclamation nor vague allusion in any WHO literature that could be interpreted as excluding pornography users. Similarly, no WHO spokesperson has ever hinted that a CSBD diagnosis excludes pornography use. Here’s the CSBD diagnosis in its entirety taken directly from the ICD-11 manual:
Compulsive sexual behaviour disorder is characterized by a persistent pattern of failure to control intense, repetitive sexual impulses or urges resulting in repetitive sexual behaviour. Symptoms may include repetitive sexual activities becoming a central focus of the person’s life to the point of neglecting health and personal care or other interests, activities and responsibilities; numerous unsuccessful efforts to significantly reduce repetitive sexual behaviour; and continued repetitive sexual behaviour despite adverse consequences or deriving little or no satisfaction from it.
The pattern of failure to control intense, sexual impulses or urges and resulting repetitive sexual behaviour is manifested over an extended period of time (e.g., 6 months or more), and causes marked distress or significant impairment in personal, family, social, educational, occupational, or other important areas of functioning. Distress that is entirely related to moral judgments and disapproval about sexual impulses, urges, or behaviours is not sufficient to meet this requirement.
Do you see anything about excluding pornography? What about excluding compulsively visiting prostitutes? Was any particular sexual behavior at all excluded? Of course not. The Prause/Klein/Kohut article cites no official WHO communication, and quotes no WHO spokesperson or working-group member. The article is little more than propaganda peppered with a handful of cherry-picked studies that are either misrepresented or not what they appear to be. (More below.)
If you have any doubts about the true nature of the Prause/Klein/Kohut press campaign, carefully read this responsible article about compulsive sexual behavior disorder (CSBD). Unlike their Slate article, this July 27, 2018 article in “SELF” goes straight to the source. It quotes official WHO spokesperson Christian Lindmeier. Lindmeier is one of only four officials WHO spokespersons listed on this page: Communications contacts in WHO headquarters – and the only WHO spokesperson to have formally commented about CSBD! The SELF article also interviewed Shane Kraus, who was at the center of the ICD-11’s Compulsive Sexual Behavior Disorder (CSBD) working group. Excerpt with Lindmeir quotes makes it clear that WHO did not reject “sex addiction”:
In regards to CSBD, the largest point of contention is whether or not the disorder should be categorized as an addiction. “There is ongoing scientific debate on whether or not the compulsive sexual behavior disorder constitutes the manifestation of a behavioral addiction,” WHO spokesperson Christian Lindmeier tells SELF. “WHO does not use the term sex addiction because we are not taking a position about whether it is physiologically an addiction or not.”
Prause/Klein/Kohut misrepresent their one and only piece of so-called “evidence”
In the following paragraph Prause/Klein/Kohut mislead the reader about “addiction” in diagnostic manuals and lie about their one and only bit of “evidence” for pornography use being excluded from the ICD-11 CSBD diagnosis:
We are also accustomed to the shock when journalists learn that “pornography addiction” is actually not recognized by any national or international diagnostic manual. With the publication of the latest International Classification of Diseases (version 11) in June, the World Health Organization once again decided not to recognize sex-film viewing as a disorder. “Pornography viewing” was considered for inclusion in the “problematic Internet use” category, but WHO decided against its inclusion because of the lack of available evidence for this disorder. (“Based on the limited current data, it would therefore seem premature to include it in the ICD-11,” the organization wrote.) The common American standard, the Diagnostic and Statistical Manual, made the same decision in their latest version as well; there is no listing for porn addiction in DSM-5.
First, neither the ICD-11 nor the APA’s DSM-5 ever uses the word “addiction” to describe an addiction – whether it be gambling addiction, heroin addiction, cigarette addiction, or you name it. Both diagnostic manuals use the word “disorder” instead of “addiction” (i.e. “gambling disorder,” “nicotine use disorder,” and so on). Thus, “sex addiction” and “porn addiction” could never have been rejected, because they were never under formal consideration in the major diagnostic manuals. Put simply, there will never be a “porn addiction” diagnosis, just as there will never be a “meth addiction” diagnosis. Yet individuals with the signs and symptoms of consistent with either a “porn addiction” or a “methamphetamine addiction” can be diagnosed using the ICD-11’s provisions.
Second, the authors’ link goes to a 2014 paper by Jon Grant, Impulse control disorders and “behavioural addictions” in the ICD-11 (2014). Before I expose Nicole Prause’s long standing misuse of the outdated Jon Grant paper, here are the indisputable facts:
(1) The Jon Grant paper is over 4 years old. In fact, 39 of the 45 neurological studies on CSB subjects listed on this page were published since the 2014 Jon Grant paper.
(2) It’s just Grant’s two cents, and not an official position paper by the World Health Organization or the CSBD work-group.
(3) Most importantly, nowhere in the paper does it say that pornography use should be excluded from CSBD. In fact, Grant says the opposite: pornography use on the internet is a form of CSB! The word “pornography” is used only once in paper and here is what Grant has to say about it:
A third key controversy in the field is whether problematic Internet use is an independent disorder. The Working Group noted that this is a heterogeneous condition, and that use of the Internet may in fact constitute a delivery system for various forms of impulse control dysfunction (e.g., pathological game playing or pornography viewing). Importantly, the descriptions of pathological gambling and of compulsive sexual behaviour disorder should note that such behaviours are increasingly seen using Internet forums, either in addition to more traditional settings, or exclusively 22, 23.
There you have it, Prause/Klein/Kohut blatantly misrepresented the only bit of “evidence” they could muster (fact-check Slate?).
However, the misrepresentation of Grant’s 2014 paper, by Prause, has been occurring for at least a year. Prause created the following image, which has been passed around pro-porn propagandists’ social media accounts. It’s a doctored screenshot of the Jon Grant paragraph I excerpted above. Counting on Twitter-induced short attention-spans, the propagandists expect you to read only what’s in the red boxes, hoping you will overlook what the paragraph actually states:
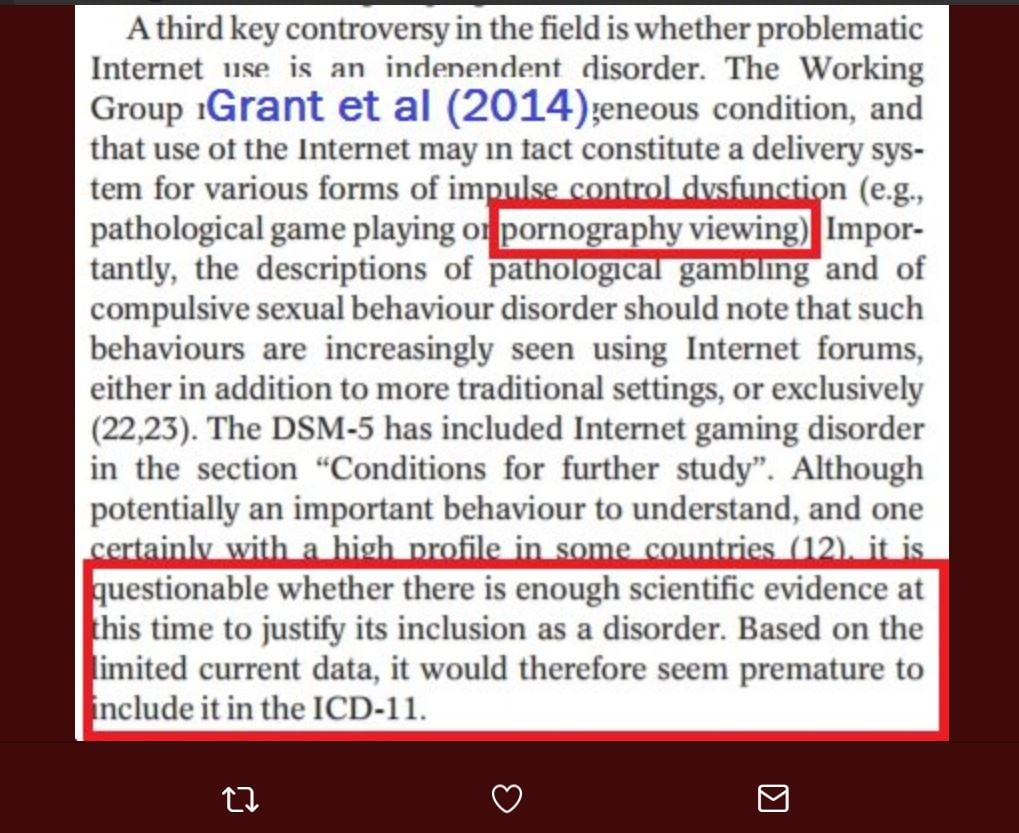
If you fell for the red-box illusion, you misread the above excerpt as:
…pornography viewing… questionable whether there is enough scientific evidence at this time to justify its inclusion as a disorder. Based on the limited current data, it would therefore seem premature to include it in the ICD-11.
Now read the entire paragraph, and you will see that Jon Grant is talking about “Internet gaming disorder,” not pornography. Grant believed it was questionable whether there was enough scientific evidence at that time to justify Internet Gaming Disorder’s inclusion as a disorder. (Incidentally, 4 years later Gaming disorder is in the ICD-11 and the scientific support for it is vast.)
A third key controversy in the field is whether problematic Internet use is an independent disorder. The Working Group noted that this is a heterogeneous condition, and that use of the Internet may in fact constitute a delivery system for various forms of impulse control dysfunction (e.g., pathological game playing or pornography viewing). Importantly, the descriptions of pathological gambling and of compulsive sexual behaviour disorder should note that such behaviours are increasingly seen using Internet forums, either in addition to more traditional settings, or exclusively 22,23.
The DSM-5 has included Internet gaming disorder in the section “Conditions for further study”. Although potentially an important behaviour to understand, and one certainly with a high profile in some countries 12, it is questionable whether there is enough scientific evidence at this time to justify its inclusion as a disorder. Based on the limited current data, it would therefore seem premature to include it in the ICD-11.
Without reading only the red squares, the above excerpt reveals that Jon Grant believes that internet pornography viewing can be an impulse control disorder that would fall under the umbrella diagnosis of “Compulsive Sexual Behavior Disorder” (CSBD). This is the exact opposite of the “red square” illusion tweeted by the propagandists.
What is Jon Grant saying 4 years later? Grant was a co-author on this 2018 paper announcing (and agreeing with) the inclusion of CSBD in the upcoming ICD-11: Compulsive sexual behaviour disorder in the ICD‐11. In a second 2018 article, “Compulsive sexual behavior: A nonjudgmental approach,” Grant says that Compulsive Sexual Behavior is also called “sex addiction” or “hypersexuality” (which have always functioned in the peer-reviewed literature as synonymous terms for any compulsive sexual behavior, including compulsive porn use):
Compulsive sexual behavior (CSB), also referred to as sexual addiction or hypersexuality, is characterized by repetitive and intense preoccupations with sexual fantasies, urges, and behaviors that are distressing to the individual and/or result in psychosocial impairment.
No wonder the propagandists such as Prause are desperately reaching back 4 years to misrepresent a Jon Grant paper. Grant’s recent 2018 paper states in the very first sentence that CSB is also called sex addiction or hypersexuality!
For an accurate account of the ICD-11, see this recent article by The Society for the Advancement of Sexual Health (SASH): “Compulsive Sexual Behaviour” has been classified by World Health Organization as Mental Health Disorder. It begins with:
Despite a few misleading rumors to the contrary, it is untrue that the WHO has rejected “porn addiction” or “sex addiction”. Compulsive sexual behavior has been called by a variety of names over the years: “hypersexuality”, “porn addiction”, “sex addiction”, “out-of-control sexual behavior” and so forth. In its latest catalogue of diseases the WHO takes a step towards legitimizing the disorder by acknowledging “Compulsive Sexual Behaviour Disorder” (CSBD) as a mental illness. According to WHO expert Geoffrey Reed, the new CSBD diagnosis “lets people know they have “a genuine condition” and can seek treatment.”
PART 2: Exposing false claims, misrepresentations, cherry-picked studies, and egregious omissions
The remainder of the Prause/Klein/Kohut article is devoted to persuading the reader that porn addiction is a myth and that internet porn use causes no problems. In addition, they imply that only the “sex negative” would dare to suggest that porn use could produce negative effects. In this section we furnish relevant Prause/Klein/Kohut excerpts followed by analysis of both the claim and references supplied to support the claim. Where appropriate we provide studies that counter their assertions.
A sample of the article’s numerous omissions:
Before we address each of the article’s major assertions, it’s important to reveal what Prause/Klein/Kohut chose to omit from their magnum opus. The lists of studies contain relevant excerpts and links to the original papers.
- Porn/sex addiction? This page lists 55 neuroscience-based studies (MRI, fMRI, EEG, neuropsychological, hormonal). They provide strong support for the addiction model as their findings mirror the neurological findings reported in substance addiction studies.
- The real experts’ opinions on porn/sex addiction? This list contains 32 recent literature reviews & commentaries by some of the top neuroscientists in the world. All support the addiction model.
- Signs of addiction and escalation to more extreme material? Over 60 studies reporting findings consistent with escalation of porn use (tolerance), habituation to porn, and even withdrawal symptoms (all signs and symptoms associated with addiction).
- Porn and sexual problems? This list contains over 40 studies linking porn use/porn addiction to sexual problems and lower arousal to sexual stimuli. The first 7 studies in the list demonstrate causation, as participants eliminated porn use and healed chronic sexual dysfunctions.
- Porn’s effects on relationships? Over 80 studies link porn use to less sexual and relationship satisfaction. As far as we know all studies involving males have reported more porn use linked to poorer sexual or relationship satisfaction.
- Porn use affecting emotional and mental health? Over 85 studies link porn use to poorer mental-emotional health & poorer cognitive outcomes.
- Porn use affecting beliefs, attitudes and behaviors? Check out individual studies – over 40 studies link porn use to “un-egalitarian attitudes” toward women and sexist views – or the summary from this 2016 meta-analysis: Media and Sexualization: State of Empirical Research, 1995–2015. Excerpt:
The goal of this review was to synthesize empirical investigations testing effects of media sexualization. The focus was on research published in peer-reviewed, English-language journals between 1995 and 2015. A total of 109 publications that contained 135 studies were reviewed. The findings provided consistent evidence that both laboratory exposure and regular, everyday exposure to this content are directly associated with a range of consequences, including higher levels of body dissatisfaction, greater self-objectification, greater support of sexist beliefs and of adversarial sexual beliefs, and greater tolerance of sexual violence toward women. Moreover, experimental exposure to this content leads both women and men to have a diminished view of women’s competence, morality, and humanity.
“But hasn’t porn use reduced rape rates?” No, rape rates have been rising in recent years: “Rape rates are on the rise, so ignore the pro-porn propaganda.” For much more, see Debunking the realyourbrainonporn (pornographyresearch.com) “Sex Offender Section”: The actual state of the research on porn use and sexual aggression, coercion & violence.
- What about sexual aggression and porn use? Another meta-analysis: A Meta‐Analysis of Pornography Consumption and Actual Acts of Sexual Aggression in General Population Studies (2015). Excerpt:
22 studies from 7 different countries were analyzed. Consumption was associated with sexual aggression in the United States and internationally, among males and females, and in cross-sectional and longitudinal studies. Associations were stronger for verbal than physical sexual aggression, although both were significant. The general pattern of results suggested that violent content may be an exacerbating factor.
“But hasn’t porn use reduced rape rates?” No, rape rates have been rising in recent years: “Rape rates are on the rise, so ignore the pro-porn propaganda.” See this page for over 100 studies linking porn use to sexual aggression, coercion & violence and an extensive critique of the often-repeated assertion that an increased availability of porn has resulted in decreased rape rates.
- What about the porn use and adolescents? Check out this list of over 280 adolescent studies, or these reviews of the literature: review#1, review2, review#3, review#4, review#5, review#6, review#7, review#8, review#9, review#10, review#11, review#12, review#13, review#14, review#15. From the conclusion of this 2012 review of the research – The Impact of Internet Pornography on Adolescents: A Review of the Research:
Increased access to the Internet by adolescents has created unprecedented opportunities for sexual education, learning, and growth. Conversely, the risk of harm that is evident in the literature has led researchers to investigate adolescent exposure to online pornography in an effort to elucidate these relationships. Collectively, these studies suggest that youth who consume pornography may develop unrealistic sexual values and beliefs. Among the findings, higher levels of permissive sexual attitudes, sexual preoccupation, and earlier sexual experimentation have been correlated with more frequent consumption of pornography…. Nevertheless, consistent findings have emerged linking adolescent use of pornography that depicts violence with increased degrees of sexually aggressive behavior.
The literature does indicate some correlation between adolescents’ use of pornography and self-concept. Girls report feeling physically inferior to the women they view in pornographic material, while boys fear they may not be as virile or able to perform as the men in these media. Adolescents also report that their use of pornography decreased as their self-confidence and social development increase. Additionally, research suggests that adolescents who use pornography, especially that found on the Internet, have lower degrees of social integration, increases in conduct problems, higher levels of delinquent behavior, higher incidence of depressive symptoms, and decreased emotional bonding with caregivers.
Prause, Ley and Klein have grossly misrepresented the current state of the research for the last few years. Now, they’ve conveniently bundled all the outlying, cherry-picked studies they regularly cite into this article. We expose the truth below. The relevant Prause/Klein/Kohut excerpts listed here are in the same sequence as in the article.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #1: Repeat after me: “Neither the DSM-5 nor the ICD-11 recognizes any addiction, only disorders”
SLATE EXCERPT: “We are also accustomed to the shock when journalists learn that “pornography addiction” is actually not recognized by any national or international diagnostic manual.”
Nice try at fooling the readers, but, again, neither the ICD-11 nor the APA’s DSM-5 ever uses the word “addiction” to describe an addiction – whether it be gambling addiction, heroin addiction, cigarette addiction or you name it. Both diagnostic manuals use the word “disorder” instead of “addiction” (i.e. “gambling disorder” “nicotine use disorder”, and so on). Thus, “sex addiction” and “porn addiction” could never have been rejected, because they were never under formal consideration in the major diagnostic manuals. Put simply, there will never be a “porn addiction” diagnosis, just as there will never be a “meth addiction” diagnosis. Yet individuals with the signs and symptoms of consistent with either a “porn addiction” or a “methamphetamine addiction” can be diagnosed using the ICD-11’s provisions.
By recognizing behavioral addictions and creating the umbrella diagnosis for compulsive sexual behaviors, the World Health Organization is coming into alignment with the American Society of Addiction Medicine (ASAM). In August, 2011 America’s top addiction experts at ASAM released their sweeping definition of addiction. From the ASAM press release:
The new definition resulted from an intensive, four‐year process with more than 80 experts actively working on it, including top addiction authorities, addiction medicine clinicians and leading neuroscience researchers from across the country. … Two decades of advancements in neurosciences convinced ASAM that addiction needed to be redefined by what’s going on in the brain.
The new definition leaves no doubt that all addictions—whether to alcohol, heroin or sex, say—are fundamentally the same. Dr. Raju Haleja, former president of the Canadian Society for Addiction Medicine and the chair of the ASAM committee that crafted the new definition, told The Fix, “We are looking at addiction as one disease, as opposed to those who see them as separate diseases. Addiction is addiction. It doesn’t matter what cranks your brain in that direction, once it has changed direction, you’re vulnerable to all addiction.” …Sex or gambling or food addiction [are] every bit as medically valid as addiction to alcohol or heroin or crystal meth.
For all practical purposes, the 2011 definition ends the debate over whether sex and porn addictions are “real addictions.” ASAM explicitly stated that sexual behavior addictions exist and must be caused by the same fundamental brain changes found in substance addictions. From the ASAM FAQs:
QUESTION: This new definition of addiction refers to addiction involving gambling, food, and sexual behaviors. Does ASAM really believe that food and sex are addicting?
ANSWER: The new ASAM definition makes a departure from equating addiction with just substance dependence, by describing how addiction is also related to behaviors that are rewarding. … This definition says that addiction is about functioning and brain circuitry and how the structure and function of the brains of persons with addiction differ from the structure and function of the brains of persons who do not have addiction. … Food and sexual behaviors and gambling behaviors can be associated with the ‘pathological pursuit of rewards’ described in this new definition of addiction.
As for the DSM, the American Psychiatric Association (APA) has so far dragged its feet on including compulsive sexual behaviors in its diagnostic manual. When it last updated the manual in 2013 (DSM-5), it didn’t formally consider “internet porn addiction,” opting instead to debate “hypersexual disorder.” The latter umbrella term for problematic sexual behavior was recommended for inclusion by the DSM-5’s own Sexuality Work Group after years of review. However, in an eleventh-hour “star chamber” session (according to a Work Group member), other DSM-5 officials unilaterally rejected hypersexuality, citing reasons that have been described as illogical.
In reaching this position, the DSM-5 disregarded formal evidence, widespread reports of the signs, symptoms and behaviors consistent with compulsion and addiction from sufferers and their clinicians, and the formal recommendation of thousands of medical and research experts at the American Society of Addiction Medicine.
Incidentally, the DSM has earned distinguished critics who object to its approach of ignoring underlying physiology and medical theory to ground its diagnoses solely in symptoms. The latter permits erratic, political decisions that defy reality. For example, the DSM once incorrectly classified homosexuality as a mental disorder.
Just prior to the DSM-5’s publication in 2013, Thomas Insel, then Director of the National Institute of Mental Health, warned that it was time for the mental health field to stop relying on the DSM. Its “weakness is its lack of validity,” he explained, and “we cannot succeed if we use DSM categories as the “gold standard.” He added, “That is why NIMH will be re-orienting its research away from DSM categories.” In other words, the NIMH would stop funding research based on DSM labels (and their absence).
It will be interesting to see what occurs with the next update of the DSM. (Note: DSM-5 did create a behavioral addiction category)
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #2: Crocodile tears
SLATE EXCERPT: Scientists and clinicians who present evidence that challenges these harm-focused narratives—and we count ourselves among that group—face serious social and political opposition to their research. It can be tough for this info to make it to the public too.
These authors spin the yarn that pro-porn advocates “face serious social and political opposition to their research” and that it can be “tough for this info to make it to the public.” Not so. In fact, pro-porn spokespersons are greatly over-represented in the press, and they have done much, often behind the scenes, to suppress opposing evidence of porn’s harms in both the popular and academic literature. (Examples)
Predictably, these authors offer no evidence of their supposed social and political difficulties. A few statistics will serve to reveal the true situation.
A Google search for “Nicole Prause” + pornography returns 16,600 results over relatively few years. Prause’s powerhouse media exposure includes quotations of her pro-porn/anti-porn addiction views in some of the most popular mainstream outlets, including Slate, Daily Beast, The Atlantic, Rolling Stone, CNN, NPR, Vice, The Sunday Times, and countless smaller outlets. Clearly Prause gets what she pays for from her glossy public relations firm. See https://web.archive.org/web/20221006103520/http://media2x3.com/category/nikky-prause/
It should be noted that Prause’s close colleague David Ley receives similar, generous press treatment. A Google search for “David Ley” + pornography returns 18,000 results – mostly because he wrote a book entitled The Myth of Sex Addiction (without ever having studied addiction in depth). A Google search for “Marty Klein” + pornography returns 41,500 results over many years.
Not only do mainstream outlets feature the views of these 3 authors, they also typically adopt these spokespersons’ narrative at face value – without seeking out the opposing views of big name academics who have published multiple neurological studies on internet porn users demonstrating evidence of porn’s harmful effects. These include Marc Potenza, Matthias Brand, Valerie Voon, Christian Laier, Simone Kühn, Jürgen Gallinat, Rudolf Stark, Tim Klucken, Ji-Woo Seok, Jin-Hun Sohn, Mateusz Gola and others.
Here’s a sample comparison. A Google search for “Matthias Brand” + pornography returns only 2,200 results. The discrepancy between coverage of distinguished academic Brand and non-academics Prause, Ley and Klein is quite revealing. Brand has authored over 340 studies, is the head of the Department of Psychology: Cognition, at the University of Duisburg-Essen, and has published more neuroscience-based studies on pornography addicts than any other researcher in the world. (See his list of his porn addiction studies here: 20 neurological studies and 4 reviews of the literature.)
Clearly, it is the serious academic researchers who are discriminated against in the press. Consequently, readers are advised to take these pro-porn authors’ narrative about the hardships they face in publicizing their pro-porn views with a healthy degree of skepticism. Journalists should do more responsible, less biased due diligence in this fractious, fractured field.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #3: A blog post by Playboy staff writer is all you got?
SLATE EXCERPT: They are also told that there is an epidemic of erectile dysfunction emerging in young men and that porn is the cause (though actual evidence suggests that there’s not).
Prause/Klein/Kohut attempt unconvincingly to debunk the well documented rise in youthful erectile dysfunction with this April, 2018 blog post by Justin Lehmiller, a regular paid contributor to Playboy Magazine. It shouldn’t surprise anyone that Lehmiller is a close ally of Prause, having featured her in at least ten of his blog posts. These and many other Lehmiller blogs perpetuate the same false narratives: porn use causes no problems and porn addiction/porn-induced sexual dysfunctions do not exist. Before we address Lehmiller’s sleight of hand regarding porn-induced sexual dysfunction, let’s examine the evidence.
Historical ED rates: Erectile dysfunction was first assessed in 1940s when the Kinsey report concluded that the prevalence of ED was less than 1% in men younger than 30 years, less than 3% in those 30–45. While ED studies on young men are relatively sparse, this 2002 meta-analysis of 6 high-quality ED studies reported that 5 of the 6 reported ED rates for men under 40 of approximately 2%. The 6th study reported figures of 7-9%, but the question used could not be compared to the 5 other studies, and did not assess chronic erectile dysfunction: “Did you have trouble maintaining or achieving an erection any time in the last year?” (Yet this anomalous study is the one that Lehmiller irresponsibly uses for comparison.)
At the end of 2006 free, streaming porn tube sites came on line and gained instant popularity. This changed the nature of porn consumption radically. For the first time in history, viewers could escalate with ease during a masturbation session without any wait.
Nine studies since 2010: Ten studies published since 2010 reveal a tremendous rise in erectile dysfunctions. This is documented in this lay article and in this peer-reviewed paper involving 7 US Navy doctors – Is Internet Pornography Causing Sexual Dysfunctions? A Review with Clinical Reports (2016). In the 10 studies, erectile dysfunction rates for men under 40 ranged from 14% to 37%, while rates for low libido ranged from 16% to 37%. Other than the advent of streaming porn (2006) no variable related to youthful ED has appreciably changed in the last 10-20 years (smoking rates are down, drug use is steady, obesity rates in males 20-40 up only 4% since 1999 – see this study).
The recent jump in sexual problems coincides with the publication of almost 40 studies linking porn use and “porn addiction” to sexual problems and lower arousal to sexual stimuli. It’s important to note that the first 7 studies in the list demonstrate causation, as participants eliminated porn use and healed chronic sexual dysfunctions (for some strange reason the Slate article failed to mention any of these 30 studies). In addition to the studies listed, this page contains articles and videos by over 140 experts (urology professors, urologists, psychiatrists, psychologists, sexologists, MDs) who acknowledge and have successfully treated porn-induced ED and porn-induced loss of sexual desire.
Lehmiller’s sleight of hand: Lehmiller carefully selected two mismatched studies, with data separated by 18 years, in an attempt to convince the reader that ED rates have always been around 8% for men under 40:
1) The “way things were study” from 1992 is the one that asked: “Did you have trouble maintaining or achieving an erection any time in the last year?” Rates of yes to this question were between 7-9%.
2) The “modern study” with 2010-12 data that asked whether men had trouble getting or keeping an erection for a period of three or more months during the last year.” This study reported the following rated of sexual functioning problems in 16-21 year old males:
- Lacked interest in having sex: 10.5%
- Difficulty reaching climax: 8.3%
- Difficulty achieving or maintaining an erection: 7.8%
Lehmiller “summarized” these findings for the vision-impaired as he tried to mislead them:
“Although these data were collected in different Western countries and the question wording differed, it’s striking how similar the figures are considering that the data were collected 20 years apart. This suggests that perhaps rates of ED aren’t on the rise among young men after all.”
Sorry Justin, but the questions are not “worded differently”; they are completely different questions. The 1992 study asked whether over the course of the last year at any point you had trouble getting it up. This includes when you were drunk, sick, just wanked three times in a row, experienced performance anxiety, whatever. I’m surprised it’s only 7-9%. In contrast, the 2010 study asked whether you had a persistent problem of erectile dysfunction over a period of three months or more: this was for 16-21 year olds, not men 39 and under!
As one recovery-forum member observed, Justin Lehmiller’s “science analysis” is Buzzfeed level clickbait, not science journalism.
But you may ask: Why are the ED rates about 8% in the 2010-2012 study, yet 14-37% in the 9 other studies published since 2010?
- First, 8% isn’t low, as that would translate in a 600%-800% increase for men under 40.
- Second, it wasn’t men under 40 – it was 16 to 21 year olds, so virtually none of them should have chronic ED. In the 1940s, the Kinsey report concluded that the prevalence of ED was less than 1% in men younger than 30 years.
- Third, unlike the other 9 studies that employed anonymous surveys, this study used face to face in-home interviews. (It’s quite possible that adolescents would be less than fully forthcoming under such circumstances.)
- The study gathered its data between August, 2010 and September, 2012. Studies reporting a significant rise in under-25 ED first appeared in 2011. More recent studies on the 25 and under crowd report higher rates (see this 2014 study on Canadian adolescents).
- Many of the other studies used the IIEF-5 or IIEF-6, which assess sexual problems on a scale, as opposed to the simple yes or no (in the past 3 months) employed in the Lehmiller’s chosen paper.
Two studies using the exact same questionnaire: 2001 vs. 2011: Before leaving this topic, it would be well to look at some of the most irrefutable research that demonstrates a radical rise in ED rates over a decade using very large samples (which increase reliability). All the men were assessed using the same (yes/no) question about ED, as part of the Global Study of Sexual Attitudes and Behavior (GSSAB), administered to 13,618 sexually active men in 29 countries. That occurred in 2001-2002.
A decade later, in 2011, the same “sexual difficulties” (yes/no) question from the GSSAB was administered to 2,737 sexually active men in Croatia, Norway and Portugal. The first group, in 2001-2002, were aged 40-80. The second group, in 2011, were 40 and under.
Based on the findings of prior studies one would predict the older men would have far higher ED scores than the younger men, whose scores should have been negligible. Not so. In just a decade, things had changed radically. The 2001-2002 ED rates for men 40-80 were about 13% in Europe. By 2011, ED rates in Europeans, ages 18-40, ranged from 14-28%!
What changed in men’s sexual environment during this time? Well, major changes were internet penetration and access to porn videos (followed by access to streaming porn in 2006, and then smartphones on which to view it). In the 2011 study on Croatians, Norwegians and Portuguese, the Portuguese had the lowest rates of ED and the Norwegians had the highest. In 2013, internet penetration rates in Portugal were only 67%, compared with 95% in Norway.
Finally, it’s important to note that author Nicole Prause has close relationships with the porn industry and is obsessed with debunking PIED, having waged a 3-year war against this academic paper, while simultaneously harassing & libeling young men who have recovered from porn-induced sexual dysfunctions. See documentation: Gabe Deem #1, Gabe Deem #2, Alexander Rhodes #1, Alexander Rhodes #2, Alexander Rhodes #3, Noah Church, Alexander Rhodes #4, Alexander Rhodes #5, Alexander Rhodes #6, Alexander Rhodes #7, Alexander Rhodes #8, Alexander Rhodes #9, Alexander Rhodes#10, Alex Rhodes#11, Gabe Deem & Alex Rhodes together#12, Alexander Rhodes#13, Alexander Rhodes #14, Gabe Deem#4, Alexander Rhodes #15.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #4: What if a meme is actually fully supported by the peer-reviewed literature?
SLATE EXCERPT: People are told that porn is toxic to marriages and that viewing it will destroy your sexual appetite.
If people are being told this, perhaps it because every single study involving males has reported that more porn use linked to poorer sexual or relationship satisfaction. In all, over 75 studies link porn use to less sexual and relationship satisfaction. From the conclusion of this meta-analysis of various other studies Pornography Consumption and Satisfaction: A Meta-Analysis (2017):
However, pornography consumption was associated with lower interpersonal satisfaction outcomes in cross-sectional surveys, longitudinal surveys, and experiments. Associations between pornography consumption and reduced interpersonal satisfaction outcomes were not moderated by their year of release or their publication status.
As for destroying sexual appetite, 37 studies link porn use or porn addiction to sexual problems and lower arousal to sexual stimuli. As examples we provide 5 of the 37 studies below:
1) The Dual Control Model – The Role Of Sexual Inhibition & Excitation In Sexual Arousal And Behavior (2007) – This was the first study on porn-induced sexual problems (by the Kinsey Institute). In an experiment employing standard video porn that had “worked” in the past, 50% of the young men now couldn’t become aroused or achieve erections with porn (average age was 29). The shocked researchers discovered that the men’s erectile dysfunction was,
related to high levels of exposure to and experience with sexually explicit materials.
The men experiencing erectile dysfunction had spent a considerable amount of time in bars and bathhouses where porn was “omnipresent” and “continuously playing.” The researchers stated:
Conversations with the subjects reinforced our idea that in some of them a high exposure to erotica seemed to have resulted in a lower responsivity to “vanilla sex” erotica and an increased need for novelty and variation, in some cases combined with a need for very specific types of stimuli in order to get aroused.
2) Brain Structure and Functional Connectivity Associated With Pornography Consumption: The Brain on Porn (2014) – A Max Planck brain scan study which found 3 significant addiction-related brain changes correlating with the amount of porn consumed. It also found that the more porn consumed the less reward circuit activity in response to brief exposure (.530 second) to vanilla porn. Lead author Simone Kühn commenting in the Max Planck press release said:
“We assume that subjects with a high porn consumption need increasing stimulation to receive the same amount of reward. That could mean that regular consumption of pornography more or less wears out your reward system. That would fit perfectly the hypothesis that their reward systems need growing stimulation.”
3) Adolescents and web porn: a new era of sexuality (2015) – This Italian study analyzed the effects of internet porn on high school seniors, co-authored by urology professor Carlo Foresta, president of the Italian Society of Reproductive Pathophysiology. The most interesting finding is that 16% of those who consume porn more than once a week report abnormally low sexual desire, as compared with 0% in non-consumers – which is exactly what you would expect for 18-year old men.
4) Patient Characteristics by Type of Hypersexuality Referral: A Quantitative Chart Review of 115 Consecutive Male Cases (2015) – A study on men (average age 41.5) with hypersexuality disorders, such as paraphilias, chronic masturbation or adultery. 27 of the men were classified as “avoidant masturbators,” meaning they masturbated to porn for one or more hours per day, or more than 7 hours per week. Findings: 71% of the men who chronically masturbated to porn reported sexual functioning problems, with 33% reporting delayed ejaculation (often a precursor to porn-induced ED).
5) “I think it has been a negative influence in many ways but at the same time I can’t stop using it”: Self-identified problematic pornography use among a sample of young Australians (2017) – Online survey of Australians, aged 15-29. Those who had ever viewed pornography (n=856) were asked an open-ended question: ‘How has pornography influenced your life?’
“Among participants who responded to the open-ended question (n=718), problematic usage was self-identified by 88 respondents. Male participants who reported problematic usage of pornography highlighted effects in three areas: on sexual function, arousal and relationships.”
The theme of this section, repeated throughout the article, is Prause/Klein/Kohut making bold yet unsupported pronouncements in the face of overwhelming empirical evidence to the contrary.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #5: Another lesson in how to manipulate data and bury findings
SLATE EXCERPT: Amazingly, the first nationally representative peer-reviewed study on sex-film viewing was only just published in 2017 in Australia. This study found that 84 percent of men and 54 percent of women had ever viewed sexual material. Overall, 3.69 percent of men (144 of 3,923) and 0.65 percent of women (28 of 4,218) in the study believed that they were “addicted” to pornography, and only half of this group reported that using pornography had any negative impact on their lives.
With pro-porn researcher Alan McKee as an author of the study named here it’s not surprising the lead headline was buried away in the study’s tables, while a cleverly worded abstract leaves the reader with the impression that only a small percentage of porn users believe porn is having a bad effects. McKee has a long history of defending porn. He authored “The Porn Report”, which an ABC analysis said was “on an ideological mission to provide an apologia for the sex industry”.
In fact, ABC revealed that: “The project on which the book is based was funded by the Australian Research Council from 2002 to 2004, and was conducted in liaison with, and with support from, the peak Australian sex industry organisation, the Eros Association, along with pornography businesses such as Gallery Entertainment and Axis Entertainment.” (emphasis supplied)
So what key finding was buried in the Australian study? 17% of males and females aged 16-30 reported that using pornography had a bad effect on them. It’s important to note that the data is 6 years old (2012), and the questions are based purely upon self-perception. Keep in mind that addicts rarely see themselves as addicted. In fact, most internet porn users are unlikely to connect symptoms to porn use unless they quit for an extended period. Here’s a screenshot of Table 5 (results):

How different would the headlines from this study have been if the authors had emphasized their key finding that nearly 1 in 5 young people believed that porn use had a “bad effect on them”? Why did they attempt to downplay this finding by ignoring it and focusing on cross-sectional results – rather than the millennial group most at risk for internet problems?
Here are a few additional reasons to take the headlines with a grain of salt:
- This was a cross-sectional representative study spanning age groups 16-69, males and females. It’s well established that young men are the primary users of internet porn. So, 25% of the men and 60% of the women had not viewed porn at least once in the last 12 months. Thus the statistics gathered minimize the problem by veiling the at-risk users.
- The single question, which asked participants if they had used porn in the last 12 months, doesn’t meaningfully quantify porn use. For example, a person who bumped into a porn site pop-up is grouped with someone who masturbates 3 times a day to hardcore porn.
- However, when the survey inquired of those who “had ever viewed porn” which ones had viewed porn in the past year, the highest percentage was the teen group. 93.4% of them had viewed in the last year, with 20-29 year olds just behind them at 88.6.
- Data was gathered between October 2012 and November 2013. Things have changed a lot in the last 4 years thanks to smartphone penetration – especially in younger users.
- Questions were asked in computer-assisted telephone interviews. It’s human nature to be more forthcoming in completely anonymous interviews, especially when interviews are about sensitive subjects such as porn use and porn-related problems.
- The questions are based purely upon self-perception. Keep in mind that addicts rarely see themselves as addicted. In fact, most internet porn users are unlikely to connect their symptoms to porn use unless they first quit for an extended period.
- The study did not employ standardized questionnaires (given anonymously), which would more accurately have assessed both porn addiction and porn’s effects on users.
What’s the data from recent studies where all participants intentionally viewed internet porn at least once in the last, say, 3-6 months, or even the last year?
- Online sexual activities: An exploratory study of problematic and non-problematic usage patterns in a sample of men (2016): This Belgian study (Leuven) found that 27.6% of subjects who had used porn in the last 3 months self-assessed their online sexual activities as problematic. The study also reports escalation, as 49% of the men reported viewing porn that was not previously interesting to them or that they once considered disgusting.
- Clinical Characteristics of Men Interested in Seeking Treatment for Use of Pornography (2016): A study on men over 18 who had viewed pornography at least once in the last 6 months. The study reported that 28% of men scored at (or above) the cutoff for possible hypersexual disorder.
- Cybersex Addiction Among College Students: A Prevalence Study (2017): In a cross-disciplinary survey of students (avg. age 23), 10.3% scored in the clinical range for cybersex addiction (19% of men and 4% of women).
- Emotion Regulation and Sex Addiction among College Students (2017): The study utilized the SAST-R “Core Scale” to assess sexual addiction. Among a sample of 337 college students, 57 (16.9 %) scored in the clinical range of sexual addiction. Breaking this down by gender, 17.8% of males and 15.5% of females in the sample surpassed the clinical cutoff.
- Who’s a Porn Addict? Examining the Roles of Pornography Use, Religiousness, and Moral Incongruence (2018): According to Dr. Joshua Grubbs, rates of porn users who answered “yes” to one of the following questions ranged from 8-20% in three diverse samples: “I believe that I am addicted to internet pornography.” or “I would call myself an internet pornography addict.”
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #6: Study reveals that self-delusion is widespread in Canada
SLATE EXCERPT: Interestingly, even among the minority of users who believe they are “addicted” to pornography, remission may be spontaneous: A study following people over time found that 100 percent of women and 95 percent of men concerned about their frequent sexual behaviors (again, not assessed clinically) no longer felt that they were addicted to sex within five years despite no documented intervention.
First spin: Contrary to the excerpt, the Canadian study did not ask participants if “they believed themselves to be addicted.” Instead, once a year (2006 to 2011) participants were asked “whether their over-involvement in the behavior had caused significant problems for them in the past 12 months”. The six behaviors were: exercise, shopping, online chat, video gaming, eating or sexual behaviors. The Slate excerpt is referring to the percentage of participants who thought they had a significant problem in ALL 5 years.
Second spin: Contrary to the excerpt all the problematic sexual behaviors were lumped together into one category – like the ICD-11 has done with CSBD. There was no “remission from porn addiction” as no participant was asked if they believed themselves to be addicted to pornography.
Third spin: Contrary to the spin, problematic sexual behaviors were the most stable excessive problem, which is remarkable as it is well established that for many libido tends to fall with age. Excerpt from study:
Our data suggested that in the vast majority of cases the reported problem behaviors were transient (Table 3). Within the subsample of respondents reporting a given problem behavior, most participants reported the given excessive behavior only once during the 5-year study period. Even the most stable problem behavior (excessive sexual behavior) was reported five times only by 5.4% of those males who reported having difficulties with this problem behavior.
The study also reveals that far more people actually have a problem than perceive they have a problem: In a clear example of self-delusion only 38 out of the 4,121 participants thought they had a problem with eating (answering ‘yes’ in 4 out of 5 years). In other words, less than 1% of Canadians believe their eating habits are causing them problems or are disordered. How could this be when 30% of adult Canadians are obese, while another 43% are overweight? Let’s not forgot the remaining 27% of Canadians who are not overweight, yet may be dealing with an eating disorder, such as anorexia nervosa or bulimia.
How could more than 99% of Canadians believe their eating habits are of no concern, when the majority of them appear to have a problem? And what does the finding really tell us about this type of study? Maybe it’s not that individuals rarely have problematic behaviors, or that troublesome behaviors fade away. Maybe, it’s exposing what is commonly acknowledged: we humans are really good at lying to ourselves.
A 2018 study on internet gamers reveals high levels of this same familiar self-delusion. 44% of gamers who met the criteria for addiction thought they had no problems: Discordance between self-report and clinical diagnosis of Internet gaming disorder in adolescents.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #7: “Not a single peer-reviewed study supports our claim, so I’ll cite a non-peer-reviewed article…in Dutch”
SLATE EXCERPT: But surely sex films are bad for relationships? In a nationally representative Dutch sample, sex-film viewing was unrelated to sexual difficulties in relationships.
In several places Prause/Klein/Kohut utilize various tactics to convince the reader that porn use has no effects of intimate relationships. They must be employing the tried and true political strategy of “attack your opponents strength,” but it won’t work. We will repeatedly cite the current state of the peer-reviewed literature and expose their subterfuge. In this excerpt suggesting that porn isn’t “bad for relationships” they cite only a single article, in Dutch, which is not peer-reviewed.
If they had a peer-reviewed study to support the assertion that porn use has no effects of relationships, they certainly would have cited it. As previously stated, over 75 studies link porn use to less sexual and relationship satisfaction. As far as we know all studies involving males (which is the majority of studies) have reported more porn use linked to poorer sexual or relationship satisfaction. While a handful of published studies correlate greater porn use in females to neutral (or better) sexual satisfaction, the vast majority most have not. See this list of 35 studies involving female subjects reporting negative effects on arousal, sexual satisfaction, and relationships.
When evaluating the research, it’s important to know that coupled females who regularly use internet porn (and can thus report on its effects) make up a relatively small percentage of all porn users. Large, nationally representative data are scarce, but the General Social Survey reported that only 2.6% of all US women had visited a “pornographic website” in the last month. The question was only asked in 2002 and 2004 (see Pornography and Marriage, 2014). Sure, porn use by younger women may have increased since 2004. Still, however, studies reporting that more porn use is correlated to greater satisfaction in women are referring to a relatively small percentage of women (perhaps only 1-2% of the female population). For example, below is a graph from one the few studies to report that more porn use is related to greater satisfaction in females.
It’s important to note that “Full” refers to males and females combined. Since the “Full” and “Men” lines are nearly identical, this tells us that almost all the frequent porn users at the far end were males. In other words the women who use 2-3 times a month or more probably comprise only 1-2% of all females. This would align with the 2004 nationally representative study mentioned above where only 2.4% of women had visited a porn site in the last month.
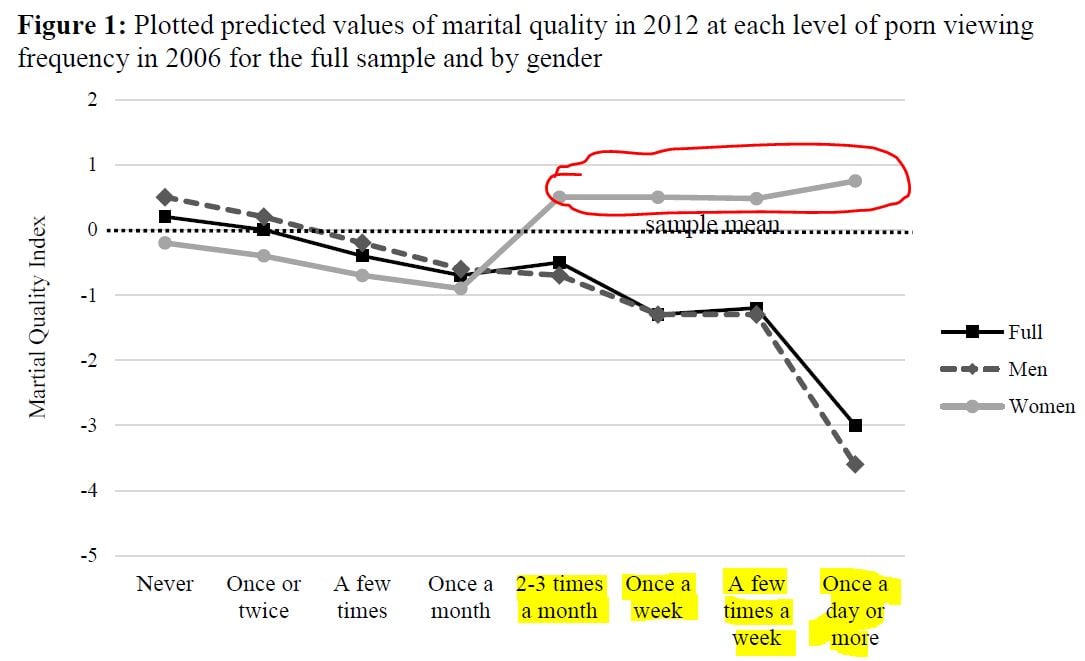
This raises several unanswered questions: What characteristics do the 1%-2% of female porn users have that leads to greater use, yet greater satisfaction? Are they into BDSM or other kinks? Are they in polyamorous relationships? Do these women possess extremely high libidos or have an addiction to porn? Whatever the reason for high levels of porn use in a tiny fraction of women, does this really tell us anything about the effects of regular porn on the other 98-99% of adult women?
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #8: The 3 studies cited do not support the claims made
SLATE EXCERPT: Similar conclusions can also be drawn from careful laboratory research, which has found that people who are worried about the frequency of their sex-film viewing actually do not struggle with the regulation of their sexual urges nor with their erectile functioning.
The above excerpt links to three studies that do not support the claims (2 of the 3 studies are by Prause). The same 3 papers and the same 2 claims are recycled from Prause’s 2016 letter (which was thoroughly debunked here: Critique of: Letter to the editor “Prause et al. (2015) the latest falsification of addiction predictions”).
First Two Studies: Winters, Christoff, & Gorzalka, 2009 and Moholy, Prause, Proudfit, Rahman, & Fong, 2015
We will begin with the first 2 studies that are cited to support the assertion that, “people who are worried about the frequency of their sex-film viewing actually do not struggle with the regulation of their sexual urges.”
The 2 studies did not assess if compulsive porn users had trouble controlling their porn use – as the excerpt falsely implies. Instead, the two studies had subjects watch a bit of porn, instructing them to attempt reduce their sexual arousal. The studies compared subjects’ scores on a sex addiction test with subjects’ ability to control their sexual arousal while watching a short clip of vanilla porn. The results for both studies were all over the place, with no clear cut correlations between the sex addiction test and the ability to inhibit one’s arousal.
The Prause/Klein/Kohut assertion is that subjects scoring highest on the sex addiction test should score lowest on controlling their arousal. Since there was no clear cut correlation in the 2 studies then “porn addiction must not exist.” Here’s why this is nonsense:
1) As stated, the studies did not assess subject’s “ability to control porn use despite negative consequences,” only transient arousal in a lab setting with a bunch of strangers in white coats lurking about.
2) The studies did not assess which participants were or were not “porn addicts” – as the researchers only used “sex addiction” questionnaires. For example, Prause’s study relied upon the CBSOB, which has zero questions about internet porn use. It only asks about “sexual activities,” or if subjects are worried about their activities (e.g., “I am worried I am pregnant,” “I gave someone HIV,” “I experienced financial problems”). Thus any correlations between scores on the CBSOB and ability to regulate arousal are irrelevant for internet porn use.
3) Most importantly: Even though neither study identified which participants were porn addicts, Prause/Klein/Kohut seem to claim that actual “porn addicts” should be the least able to control their sexual arousal while viewing porn. Yet why would they think porn addicts should have “higher arousal’ when Prause et al., 2015 reported that more frequent porn users had less brain activation to vanilla porn than did controls? (Incidentally, another EEG study similarly found that greater porn use in women correlated with less brain activation to porn.) The findings of Prause et al. 2015 align with Kühn & Gallinat (2014), which found that more porn use correlated with less brain activation in response to pictures of vanilla porn, and with Banca et al. 2015, which found faster habituation to sexual images in porn addicts.
It is not uncommon for frequent porn users to develop tolerance, which is the need for greater stimulation in order to achieve the same level of arousal. Vanilla porn can become boring. A similar phenomenon occurs in substance abusers who require bigger “hits” to achieve the same high. With porn users, greater stimulation is often achieved by escalating to new or extreme genres of porn. A recent study found that such escalation is very common in today’s internet porn users. 49% of the men surveyed had viewed porn that “was not previously interesting to them or that they considered disgusting.” In fact, multiple studies have reported findings consistent habituation or escalation in frequent porn users – an effect entirely consistent with the addiction model.
Key point: The authors’ entire claim rests upon the unsupported prediction that “porn addicts” should experience greater sexual arousal to static images of vanilla porn, and thus less ability to control their arousal. Yet the prediction that compulsive porn users would experience greater arousal to vanilla porn and greater sexual desire has repeatedly been refuted by several lines of research:
- Over 25 studies refute the claim that sex and porn addicts “have high sexual desire.”
- Over 35 studies link porn use to lower sexual arousal or sexual dysfunctions with sex partners.
- Over 75 studies link porn use with lower sexual and relationship satisfaction.
Relevant: In another example of agenda-driven bias, Prause claimed that her 2015 results of lower brain activation in response to vanilla porn had completely “debunked porn addiction.” 10 peer-reviewed papers disagree with Prause. All say that Prause et al., 2015 actually found desensitization/habituation in frequent porn users (which is consistent with the addiction model): Peer-reviewed critiques of Prause et al., 2015
The Third Study (Prause & Pfaus 2015):
A single paper, co-authored by Nicole Prause, was cited to support the claim that porn use has no effects on sexual functioning (“…..nor with their erectile functioning.“) Before we address this heavily criticized paper (Prause & Pfaus), let’s review the evidence in support of porn-induced sexual dysfunctions.
As detailed in Excerpt #3 above, nine studies published since 2010 reveal a tremendous rise in erectile dysfunction. This is documented in this lay article and in this peer-reviewed paper involving 7 US Navy doctors: Is Internet Pornography Causing Sexual Dysfunctions? A Review with Clinical Reports (2016). Prior to 2001 erectile dysfunction rates for men under 40 hovered around 2-3%. Since 2010 ED rates range from 14% to 37%, while rates for low libido ranged from 16% to 37%. Other than the advent of streaming porn no variable related to youthful ED has appreciably changed in the last 10-20 years.
The recent jump in sexual problems coincides with the publication of 28 studies linking porn use and “porn addiction” to sexual problems and lower arousal to sexual stimuli. It’s important to note that the first 5 studies in the list demonstrate causation, as participants eliminated porn use and healed chronic sexual dysfunctions. For some strange reason the Slate article fails to mention any of these 26 studies.
In addition to the studies listed, this page contains articles and videos by over 130 experts (urology professors, urologists, psychiatrists, psychologists, sexologists, MDs) who acknowledge, and have successfully treated, porn-induced ED and porn-induced loss of sexual desire. In addition tens of thousands of young men have reported curing chronic sexual dysfunction by removing a single variable: porn. (See these pages for a few thousand such recovery stories: Rebooting accounts 1, Rebooting accounts 2, Rebooting Accounts 3, Short PIED recovery stories.)
Prause & Pfaus did not support its claims: I provide the formal critique by Richard Isenberg, MD and a very extensive lay critique, followed by my comments and excerpts from Dr. Isenberg’s critique:
- In the same journal as the paper: Letter to the editor by Richard A. Isenberg MD (2015)
- Very extensive lay critique: Nothing Adds Up in Dubious Study: Youthful Subjects’ ED Left Unexplained (2015)
Prause & Pfaus 2015 wasn’t a study on men with ED. It wasn’t a study at all. Instead, Prause claimed to have gathered data from four of her earlier studies, none of which addressed erectile dysfunction. It’s disturbing that this paper by Nicole Prause and Jim Pfaus passed peer-review as the data in their paper did not match the data in the underlying four studies on which the paper claimed to be based. The discrepancies are not minor gaps, but gaping holes that cannot be plugged. In addition, the paper made several claims that were false or not supported by their data.
We begin with false claims made by both Nicole Prause and Jim Pfaus. Many journalists’ articles about this study claimed that porn use led to better erections, yet that’s not what the paper found. In recorded interviews, both Nicole Prause and Jim Pfaus falsely claimed that they had measured erections in the lab, and that the men who used porn had better erections. In the Jim Pfaus TV interview Pfaus states:
We looked at the correlation of their ability to get an erection in the lab.
We found a liner correlation with the amount of porn they viewed at home, and the latencies which for example they get an erection is faster.
In this radio interview Nicole Prause claimed that erections were measured in the lab. The exact quote from the show:
The more people watch erotica at home they have stronger erectile responses in the lab, not reduced.
Yet this paper did not assess erection quality in the lab or “speed of erections.” The paper only claimed to have asked guys to rate their “arousal” after briefly viewing porn (and it’s not clear from the underlying papers that this simple self-report was even asked of all subjects). In any case, an excerpt from the paper itself admitted that:
No physiological genital response data were included to support men’s self-reported experience”
In other words, no actual erections were tested or measured in the lab, which means that no such data or conclusions were peer-reviewed!
In a second unsupported claim, lead author Nicole Prause tweeted several times about the study, letting the world know that 280 subjects were involved, and that they had “no problems at home.” However, the four underlying studies contained only 234 male subjects, so “280” is way off.
A third unsupported claim: Dr. Isenberg’s Letter to the Editor (linked to above), which raised multiple substantive concerns highlighting the flaws in Prause & Pfaus , wondered how it could be possible for Prause & Pfaus to have compared different subjects’ arousal levels when three different types of sexual stimuli were used in the 4 underlying studies. Two studies used a 3-minute film, one study used a 20-second film, and one study used still images. It’s well established that films are far more arousing than photos, so no legitimate research team would group these subjects together to make claims about their responses. What’s shocking is that in their paper authors Prause and Pfaus unaccountably claim that all 4 studies used sexual films:
“The VSS presented in the studies were all films.”
This statement is false, as clearly revealed in Prause’s own underlying studies. This is the first reason why Prause and Pfaus cannot claim that their paper assessed “arousal.” You must use the same stimulus for each subject to compare all subjects.
A fourth unsupported claim: Dr. Isenberg also asked how Prause & Pfaus 2015 could compare different subjects’ arousal levels when only 1 of the 4 underlying studies used a 1 to 9 scale. One used a 0 to 7 scale, one used a 1 to 7 scale, and one study did not report sexual arousal ratings. Once again Prause and Pfaus inexplicably claim that:
“Men were asked to indicate their level of “sexual arousal” ranging from 1 “not at all” to 9 “extremely.”
This statement, too, is false, as the underlying papers show. This is the second reason why Prause and Pfaus cannot claim that their paper assessed “arousal” ratings in men. A study must use the same rating scale for each subject to compare the subjects’ results. In summary, all the Prause-generated headlines and claims about porn use improving erections or arousal, or anything else, are unsupported by her research.
Authors Prause and Pfaus also claimed they found no relationship between erectile functioning scores and the amount of porn viewed in the last month. As Dr. Isenberg pointed out:
Even more disturbing is the total omission of statistical findings for the erectile function outcome measure. No statistical results whatsoever are provided. Instead the authors ask the reader to simply believe their unsubstantiated statement that there was no association between hours of pornography viewed and erectile function. Given the authors’ conflicting assertion that erectile function with a partner may actually be improved by viewing pornography the absence of statistical analysis is most egregious.
As is customary when a letter critical of a study is published, the study’s authors were given a chance to respond. Prause’s pretentious response entitled “Red Herring: Hook, Line, and Stinker” not only evades Isenberg’s points (and Gabe Deem’s), it contains several new misrepresentations and several transparently false statements. In fact, Prause’s reply is little more than smoke, mirrors, groundless insults, and falsehoods. This extensive critique by Gabe Deem exposes the Prause and Pfaus response for what it is: A critique of the Prause & Pfaus response to Richard Isenberg’s letter.
Summary: The 2 core claims made by Klein/Kohut/Prause remain unsupported:
- Prause & Pfaus failed to provide data for its core claim that porn use was not related to scores on an erection questionnaire (IIEF).
- Prause & Pfaus failed to explain how its authors could reliably assess “arousal” when the 4 underlying studies used different stimuli (still images vs. films), and use no scale or very different number scales (1-7, 1-9, 0-7, no scale).
If Prause and Pfaus had answers to the above concerns, they would have put them in their response to Dr. Isenberg. They didn’t.
Finally, Jim Pfaus is on the editorial board of The Journal of Sexual Medicine and spends considerable effort attacking the concept of porn-induced sexual dysfunctions. Co-author Nicole Prause is obsessed with debunking PIED, having waged a 3-year war against this academic paper, while simultaneously harassing and libeling young men who have recovered from porn-induced sexual dysfunctions. See documentation: Gabe Deem #1, Gabe Deem #2, Alexander Rhodes #1, Alexander Rhodes #2, Alexander Rhodes #3, Noah Church, Alexander Rhodes #4, Alexander Rhodes #5, Alexander Rhodes #6, Alexander Rhodes #7, Alexander Rhodes #8, Alexander Rhodes #9, Alexander Rhodes#10, Gabe Deem & Alex Rhodes together, Alexander Rhodes#11, Alexander Rhodes #12, Alexander Rhodes #13, Alexander Rhodes #14.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #9: When confronted with hundreds of studies linking porn use to negative outcomes just shout “correlation is not causation”
SLATE EXCERPT: However, a core problem with this area of research is that the overwhelming majority of studies are cross-sectional, meaning they just ask about your life as it is now. This means that they cannot show causality. Remember the old “correlation is not causation” principle from science class? If your marriage is not going well or you stopped being intimate years ago, chances are good that someone in that relationship is masturbating to sate their unfulfilled sexual desire.
Translation: “You are getting very, very sleepy…your eyelids are getting heavy… no matter what 58 studies on porn use relationships reveal, it’s really masturbation…. You are now asleep.… it can’t be porn….porn is good for you…. it must be masturbation…. Go deeper asleep, deeper asleep.”
As recounted under excerpt #14, the strategy fashioned by Prause and David Ley is to blame masturbation for the myriad problems related to porn use. Here and in #14 below, Prause/Klein/Kohut pick up this fabricated talking point and try to blame masturbation for the results from over 60 studies linking porn use to less sexual and relationship satisfaction. After Prause and Ley constructed the “porn is never the problem” tactic to explain chronic ED in otherwise healthy young men, their close ally, Jim Pfaus, repeatedly asserted that porn-induced ED is a myth, and that post-ejaculation refractory periods are the real cause of these young men’s ED. When asked about the fact that it takes 6-24 months of no porn to regain erections, Pfaus goes silent. That’s some “refractory period,” eh? (See this article exposing “their blame anything but porn” campaign: Sexologists deny porn-induced ED by claiming masturbation is the problem (2016).)
On to the “correlation doesn’t equal causation” mantra that any 7th grader can recite. When confronted with hundreds of studies linking porn use to negative outcomes, a common tactic by pro-porn PhDs is to claim that “no causation has been demonstrated.” The reality is that when it comes to psychological and medical studies, very little research reveals causation directly. For example, all studies on the relationship between lung cancer and cigarette smoking in humans are correlative. Yet cause and effect are now clear to everyone but the tobacco lobby.
For ethical reasons, researchers are usually precluded from constructing experimental research designs that would reveal definitively whether pornography causes certain harms. Therefore, they use correlational models. Over time, when a significant body of correlational studies is amassed in any given research area, there comes a point where the body of evidence can be said to demonstrate a point of theory, despite a lack of the ideal, but often unethical to conduct, experimental studies.
Put another way, no single correlation study may ever provide a “smoking gun” in an area of study, but the converging evidence of multiple correlational studies can establish cause and effect. When it comes to porn use, nearly every study published is correlative.
To “prove” that porn use is causing erectile dysfunction, relationship problems, emotional problems or addiction-related brain changes you would have to have two large groups of identical twins separated at birth. Make sure one group never watches porn. Make sure that every individual in the other group watches the exact same type of porn, for the exact same hours, at the exact same age. And continue the experiment for 30 years or so, followed by assessment of the differences.
Alternatively, research attempting to demonstrate causation could be done using the following 3 methods:
- Eliminate the variable whose effects you wish to measure. Specifically, have porn users stop, and assess any changes weeks, months (years?) later. This is exactly what is occurring as thousands of young men stop porn as a way to alleviate chronic non-organic erectile dysfunction and other symptoms (caused by porn use).
- Perform longitudinal studies, which means following subjects over a period of time to see how changes in porn use (or levels of porn use) relate to various outcomes. For example, correlate levels of porn use with rates of divorce over years (asking other questions to control for other possible variables).
- Expose willing participants to pornography and measure various outcomes. For example, assess subjects’ ability to delay gratification both before and after exposure to porn in a lab setting.
Below we list studies that have employed these 3 methods: elimination porn use, longitudinal studies, exposure to pornography in a lab. All of the results strongly suggest that porn use leads to negative outcomes.
Section #1: Studies where participants eliminated porn use:
The first 7 studies in this section demonstrate porn use causing sexual problems as participants eliminated porn use and healed chronic sexual dysfunctions. Thus, the debate about whether porn-induced sexual dysfunctions exist has been settled for some time now.
1) Is Internet Pornography Causing Sexual Dysfunctions? A Review with Clinical Reports (2016): An extensive review of the literature related to porn-induced sexual problems. Co-authored by 7 US Navy doctors (urologists, psychiatrists, and an MD with PhD in neuroscience), the review provides the latest data revealing a tremendous rise in youthful sexual problems. It also reviews the neurological studies related to porn addiction and sexual conditioning via internet porn. The authors provide 3 clinical reports of men who developed porn-induced sexual dysfunctions. Two of the three men healed their sexual dysfunctions by eliminating porn use. The third man experienced little improvement as he was unable to abstain from porn use.
2) Male masturbation habits and sexual dysfunctions (2016): Authored by a French psychiatrist and president of the European Federation of Sexology. The paper revolves around his clinical experience with 35 men who developed erectile dysfunction and/or anorgasmia, and his therapeutic approaches for helping them. The author states that most of his patients used porn, with a quarter of them being addicted to porn. The abstract points to internet porn as the primary cause of patients’ problems. 19 of the 35 men saw significant improvements in sexual functioning. The other men either dropped out of treatment or were still trying to recover.
3) Unusual masturbatory practice as an etiological factor in the diagnosis and treatment of sexual dysfunction in young men (2014): One of the 4 case studies in this paper reports on a man with porn-induced sexual problems (low libido, fetishes, anorgasmia). The sexual intervention called for a 6-week abstinence from porn and masturbation. After 8 months the man reported increased sexual desire, successful sex and orgasm, and enjoying “good sexual practices. This is the first peer-reviewed chronicling of a recovery from porn-induced sexual dysfunctions.
4) How difficult is it to treat delayed ejaculation within a short-term psychosexual model? A case study comparison (2017): This is a report on two “composite cases” illustrating the etiology and treatments for delayed ejaculation (anorgasmia). “Patient B” represented multiple young men treated by the therapist. Patient B’s “porn use had escalated into harder material,” “as is often the case.” The paper says that porn-related delayed ejaculation is not uncommon, and on the rise. The author calls for more research on porn’s effects on sexual functioning. Patient B’s delayed ejaculation was healed after 10 weeks of no porn.
5) Situational Psychogenic Anejaculation: A Case Study (2014): The details reveal a case of porn-induced anejaculation. The husband’s only sexual experience prior to marriage was frequent masturbation to pornography (where he was able to ejaculate). He also reported sexual intercourse as less arousing than masturbation to porn. The key piece of information is that “re-training” and psychotherapy failed to heal his anejaculation. When those interventions failed, therapists suggested a complete ban on masturbation to porn. Eventually this ban resulted in successful sexual intercourse and ejaculation with a partner for the first time in his life.
6) Pornography Induced Erectile Dysfunction Among Young Men (2019) – This paper explores the phenomenon of pornography induced erectile dysfunction (PIED), with 12 cases studies. Several men healed porn-induced ED by eliminating porn use.
7) Hidden in Shame: Heterosexual Men’s Experiences of Self-Perceived Problematic Pornography Use (2019) – Interviews of 15 male porn users. Several of the men reported porn addiction, escalation of use and porn-induced sexual problems. One of the compulsive porn users significantly improved his erectile function during sexual encounters by severely limiting his porn use.
8) How Abstinence Affects Preferences (2016) [preliminary results]. Results of the Second Wave – Main Findings:
– Abstaining from pornography and masturbation increases the ability to delay rewards
– Participating in a period of abstinence renders people more willing to take risks
– Abstinence renders people more altruistic
– Abstinence renders people more extroverted, more conscientious, and less neurotic
9) A Love That Doesn’t Last: Pornography Consumption and Weakened Commitment to One’s Romantic Partner (2012): Subjects attempted to abstain from porn use (only 3 weeks). Comparing this group with control participants, those who continued using pornography reported lower levels of commitment than controls. What might have occurred if they had attempted to abstain for 3 months instead of 3 weeks?
10) Trading Later Rewards for Current Pleasure: Pornography Consumption and Delay Discounting (2015): The more pornography that participants consumed, the less able they were to delay gratification. This unique study also had porn users attempt to reduce porn use for 3 weeks. The study found that continued porn use was causally related to greater inability to delay gratification (note that the ability to delay gratification is a function of the brain’s prefrontal cortex).
Section #2: Longitudinal studies:
All but two of the longitudinal studies examined the effects of porn use on intimate relationships
1) Early adolescent boys’ exposure to internet pornography: Relationships to pubertal timing, sensation seeking, and academic performance (2014): An increase in porn use was followed by a decrease in academic performance 6 months later.
2) Adolescents’ Exposure to Sexually Explicit Internet Material and Sexual Satisfaction: A Longitudinal Study (2009). Excerpt: Between May 2006 and May 2007, we conducted a three-wave panel survey among 1,052 Dutch adolescents aged 13–20. Structural equation modeling revealed that exposure to SEIM consistently reduced adolescents’ sexual satisfaction. Lower sexual satisfaction (in Wave 2) also increased the use of SEIM (in Wave 3).
3) Does Viewing Pornography Reduce Marital Quality Over Time? Evidence from Longitudinal Data (2016). Excerpt: This study is the first to draw on nationally representative, longitudinal data (2006-2012 Portraits of American Life Study) to test whether more frequent pornography use influences marital quality later on and whether this effect is moderated by gender. In general, married persons who more frequently viewed pornography in 2006 reported significantly lower levels of marital quality in 2012, net of controls for earlier marital quality and relevant correlates. Pornography’s effect was not simply a proxy for dissatisfaction with sex life or marital decision-making in 2006. In terms of substantive influence, frequency of pornography use in 2006 was the second strongest predictor of marital quality in 2012.
4) Till Porn Do Us Part? Longitudinal Effects of Pornography Use on Divorce, (2016). The study used nationally representative General Social Survey panel data collected from thousands of American adults. Excerpt: Beginning pornography use between survey waves nearly doubled one’s likelihood of being divorced by the next survey period, from 6 percent to 11 percent, and nearly tripled it for women, from 6 percent to 16 percent. Our results suggest that viewing pornography, under certain social conditions, may have negative effects on marital stability.
5) Internet pornography and relationship quality: A longitudinal study of within and between partner effects of adjustment, sexual satisfaction and sexually explicit internet material among newly-weds (2015). Excerpt: The data from a considerable sample of newlyweds showed that SEIM use has more negative than positive consequences for husbands and wives. Importantly, husbands’ adjustment decreased SEIM use over time and SEIM use decreased adjustment. Furthermore, more sexual satisfaction in husbands predicted a decrease in their wives’ SEIM use one year later, while wives’ SEIM use did not change their husbands’ sexual satisfaction.
6) Pornography Use and Marital Separation: Evidence from Two-Wave Panel Data (2017). Excerpt: analyses showed that married Americans who viewed pornography at all in 2006 were more than twice as likely as those who did not view pornography to experience a separation by 2012, even after controlling for 2006 marital happiness and sexual satisfaction as well as relevant sociodemographic correlates. The relationship between pornography use frequency and marital separation, however, was technically curvilinear.
7) Are Pornography Users More Likely to Experience A Romantic Breakup? Evidence from Longitudinal Data (2017). Excerpt: analyses demonstrated that Americans who viewed pornography at all in 2006 were nearly twice as likely as those who never viewed pornography to report experiencing a romantic breakup by 2012, even after controlling for relevant factors such as 2006 relationship status and other sociodemographic correlates. Analyses also showed a linear relationship between how frequently Americans viewed pornography in 2006 and their odds of experiencing a breakup by 2012.
8) Relationships between Exposure to Online Pornography, Psychological Well-Being and Sexual Permissiveness among Hong Kong Chinese Adolescents: a Three-Wave Longitudinal Study (2018): This longitudinal study found that porn use was related to depression, lower life satisfaction and permissive sexual attitudes.
Section #3: Experimental exposure to pornography:
1) Effect of Erotica on Young Men’s Aesthetic Perception of Their Female Sexual Partners (1984). Excerpt: After exposure to beautiful females, mates’ aesthetic value fell significantly below assessments made after exposure to unattractive females; this value assumed an intermediate position after control exposure. Changes in mates’ aesthetic appeal did not correspond with changes in satisfaction with mates, however.
2) Effects of Prolonged Consumption of Pornography on Family Values (1988). Excerpt: Exposure prompted, among other things, greater acceptance of pre- and extramarital sex and greater tolerance of nonexclusive sexual access to intimate partners. Exposure lowered the evaluation of marriage, making this institution appear less significant and less viable in the future. Exposure also reduced the desire to have children and promoted the acceptance of male dominance and female servitude. With few exceptions, these effects were uniform for male and female respondents as well as for students and nonstudents.
3) Pornography’s Impact on Sexual Satisfaction (1988). Excerpt: Male and female students and nonstudents were exposed to videotapes featuring common, nonviolent pornography or innocuous content. Exposure was in hourly sessions in six consecutive weeks. In the seventh week, subjects participated in an ostensibly unrelated study on societal institutions and personal gratifications. [Porn use] strongly impacted self-assessment of sexual experience. After consumption of pornography, subjects reported less satisfaction with their intimate partners—specifically, with these partners’ affection, physical appearance, sexual curiosity, and sexual performance proper. In addition, subjects assigned increased importance to sex without emotional involvement. These effects were uniform across gender and populations.
4) Influence of popular erotica on judgments of strangers and mates (1989). Excerpt: In Experiment 2, male and female subjects were exposed to opposite sex erotica. In the second study, there was an interaction of subject sex with stimulus condition upon sexual attraction ratings. Decremental effects of centerfold exposure were found only for male subjects exposed to female nudes. Males who found the Playboy-type centerfolds more pleasant rated themselves as less in love with their wives.
5) Pornographic picture processing interferes with working memory performance (2013): German scientists have discovered that Internet erotica can diminish working memory. In this porn-imagery experiment, 28 healthy individuals performed working-memory tasks using 4 different sets of pictures, one of which was pornographic. Participants also rated the pornographic pictures with respect to sexual arousal and masturbation urges prior to, and after, pornographic picture presentation. Results showed that working memory was worst during the porn viewing and that greater arousal augmented the drop.
6) Sexual Picture Processing Interferes with Decision-Making Under Ambiguity (2013): Study found that viewing pornographic imagery interfered with decision making during a standardized cognitive test. This suggests porn might affect executive functioning, which is a set of mental skills that help you get things done. These skills are controlled by an area of the brain called the prefrontal cortex.
7) Getting stuck with pornography? Overuse or neglect of cybersex cues in a multitasking situation is related to symptoms of cybersex addiction (2015): Subjects with a higher tendency towards porn addiction performed more poorly of executive functioning tasks (which are under the auspices of the prefrontal cortex).
8) Executive Functioning of Sexually Compulsive and Non-Sexually Compulsive Men Before and After Watching an Erotic Video (2017): Exposure to porn affected executive functioning in men with “compulsive sexual behaviors,” but not healthy controls. Poorer executive functioning when exposed to addiction-related cues is a hallmark of substance disorders (indicating both altered prefrontal circuits and sensitization).
9) Exposure to Sexual Stimuli Induces Greater Discounting Leading to Increased Involvement in Cyber Delinquency Among Men (Cheng & Chiou, 2017): In two studies exposure to visual sexual stimuli resulted in: 1) greater delayed discounting (inability to delay gratification), 2) greater inclination to engage in cyber-delinquency, 3) greater inclination to purchase counterfeit goods and hack someone’s Facebook account. Taken together this indicates that porn use increases impulsivity and may reduce certain executive functions (self-control, judgment, foreseeing consequences, impulse control).
By the way, over 80 internet addiction studies have employed “longitudinal” and “remove the variable” methodologies. All strongly suggesting that internet use can cause mental/emotional problems, addiction-related brain changes, and other negative effects in some users.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #10: Prause/Klein/Kohut cherry-pick 5% of subjects from 1 of the 58 studies linking porn use to poorer relationships
SLATE EXCERPT: Longitudinal studies following people over time at least show if sex-film viewing occurred before a proposed effect, which is necessary to suggest that sex films caused the effect. For example, one longitudinal study showed that, on average, sex-film viewing increased the risk of relationship loss later. Till Porn Do Us Part? A Longitudinal Examination of Pornography Use and Divorce. However, another study found that married Americans with the highest frequencies of sex-film use actually were at the lowest risk for losing their relationship (a nonlinear effect).
The tactic here is to fool the reader into thinking that the research investigating porn’s effects on relationships is conflicted. They do this by acknowledge the existence of one study linking porn to relationship troubles (out of the 75 studies linking porn use to poorer relationship), followed by cherry-picking the only study reporting an outlier result – for a small percentage of its subjects (5% of subjects).
The study with an outlier finding for less than 5% of the subjects is “Pornography Use and Marital Separation: Evidence from Two-Wave Panel Data (2017)” – Excerpt from the abstract:
Drawing on data from the 2006 and 2012 waves of the nationally representative Portraits of American Life Study, this article examined whether married Americans who viewed pornography in 2006, either at all or in greater frequencies, were more likely to experience a marital separation by 2012. Binary logistic regression analyses showed that married Americans who viewed pornography at all in 2006 were more than twice as likely as those who did not view pornography to experience a separation by 2012, even after controlling for 2006 marital happiness and sexual satisfaction as well as relevant sociodemographic correlates. The relationship between pornography use frequency and marital separation, however, was technically curvilinear. The likelihood of marital separation by 2012 increased with 2006 pornography use to a point and then declined at the highest frequencies of pornography use.
The actual results. Grouped together, the pornography users (either the men or the women) were more than twice as likely to experience a marital separation 6 years later. Specifically, for 95% of the subjects, porn use in 2006 was related with an increased likelihood of marital separation in 2012. However, once porn use frequency reached several times a week or more (only 5% of subjects) the likelihood of separation was about the same as for those who didn’t use porn.
As pointed out under excerpt #7 correlations at the far end of the bell curve may not predict results for the vast majority of porn users. In this mixed bag of 2-5% of frequent users we may find a much higher percentage of couples who identify as swingers or polyamorous. They may have open marriages. Maybe the couple has an understanding that the partner can use as much porn as desired, but divorce is never an option. Whatever the reason for high levels of porn use in one or both partners, it’s clear from this study and all the rest, that the outliers don’t line up with the vast majority of couples.
By the way, all the other longitudinal studies confirm that porn use is related poorer relationship outcomes.
- A Love That Doesn’t Last: Pornography Consumption and Weakened Commitment to One’s Romantic Partner (2012): Subjects attempted to abstain from porn use (only 3 weeks). Comparing this group with control participants, those who continued using pornography reported lower levels of commitment than controls. What might have occurred if they had attempted to abstain for 3 months instead of 3 weeks?
- Internet pornography and relationship quality: A longitudinal study of within and between partner effects of adjustment, sexual satisfaction and sexually explicit internet material among newly-weds (2015). Excerpt: The data from a considerable sample of newlyweds showed that SEIM use has more negative than positive consequences for husbands and wives. Importantly, husbands’ adjustment decreased SEIM use over time and SEIM use decreased adjustment. Furthermore, more sexual satisfaction in husbands predicted a decrease in their wives’ SEIM use one year later, while wives’ SEIM use did not change their husbands’ sexual satisfaction.
- Does Viewing Pornography Reduce Marital Quality Over Time? Evidence from Longitudinal Data (2016). Excerpt: This study is the first to draw on nationally representative, longitudinal data (2006-2012 Portraits of American Life Study) to test whether more frequent pornography use influences marital quality later on and whether this effect is moderated by gender. In general, married persons who more frequently viewed pornography in 2006 reported significantly lower levels of marital quality in 2012, net of controls for earlier marital quality and relevant correlates. Pornography’s effect was not simply a proxy for dissatisfaction with sex life or marital decision-making in 2006. In terms of substantive influence, frequency of pornography use in 2006 was the second strongest predictor of marital quality in 2012.
- Are Pornography Users More Likely to Experience A Romantic Breakup? Evidence from Longitudinal Data (2017). Excerpt: analyses demonstrated that Americans who viewed pornography at all in 2006 were nearly twice as likely as those who never viewed pornography to report experiencing a romantic breakup by 2012, even after controlling for relevant factors such as 2006 relationship status and other sociodemographic correlates. Analyses also showed a linear relationship between how frequently Americans viewed pornography in 2006 and their odds of experiencing a breakup by 2012.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #11: Oops. Prause/Klein/Kohut unknowingly cite a study that supports the addiction model
SLATE EXCERPT: Having a strong brain response to sex films in the lab also predicts a stronger drive to have sex with a partner months later.
How the study linked to supports this talking point is anyone’s guess. Perhaps they think the reader will misread this as “porn viewing leads to greater desire for sex with a real person that is sustained for several months.” But that’s not what the study reported.
This was a study about mechanisms behind compulsive behaviors (overeating and compulsive sexual behaviors). The study found that greater cue-reactivity to porn correlated with greater cravings to have sex and masturbate six months later. The study did not assess “desire to be with a partner”. It only assessed cravings to masturbate and have sex, which wasn’t limited to a single partner. The study found similar results for food: subjects with greater cue-reactivity to images of enticing food gained the most weight over the next six months. From the study’s abstract:
These findings suggest that heightened reward responsivity in the brain to food and sexual cues is associated with indulgence in overeating and sexual activity, respectively, and provide evidence for a common neural mechanism associated with appetitive behaviors.
This study supports the addiction model, as subjects with the greatest cue-reactivity (reward center activity) in response to porn experienced greater cravings to act out six months later. It appears these individuals had become sensitized to pornography, which manifested as both cue-reactivity and cravings to use. Addiction researchers view sensitization as the core brain change that leads to compulsive consumption and ultimately addiction. (See “The incentive sensitization theory of addiction”)
Sensitized pathways can be thought of as Pavlovian conditioning on turbos. When activated by thoughts or triggers, sensitized pathways blast the reward circuit, firing up hard-to-ignore cravings. Several recent brain studies on porn users assessed sensitization, and all reported the same brain response as seen in alcoholics and drug addicts. As of 2018 some 25 studies have reported findings consistent with sensitization (cue-reactivity or cravings) in porn users and porn addicts: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25.
It’s important to note that sensitization is not a sign of true libido or desire to get close to a partner. Instead, it’s evidence of hyper-sensitivity to memories or cues related to the behavior. For example, cues – such as turning on the computer, seeing a pop-up, or being alone – may trigger intense, hard to ignore cravings to view porn. Studies reveal that compulsive porn users can have greater cue-reactivity or cravings for porn, and yet experience low sexual desire and erectile dysfunction with real partners. For example, in the Cambridge University brain scan studies on porn addicts the subjects had greater brain activation to porn, but many reported arousal/erectile problems with partners. From the 2014 Cambridge study:
[Compulsive sexual behaviour] subjects reported that as a result of excessive use of sexually explicit materials…..they experienced diminished libido or erectile function specifically in physical relationships with women (although not in relationship to the sexually explicit material).
Then we have the Nicole Prause 2013 EEG study which she touted in the media as evidence against the existence of porn/sex addiction: Sexual Desire, not Hypersexuality, is Related to Neurophysiological Responses Elicited by Sexual Images (Steele et al., 2013). Not so. Steele et al. 2013 actually lends support to the existence of both porn addiction and porn use down-regulating sexual desire. How so? The study reported higher EEG readings (relative to neutral pictures) when subjects were briefly exposed to pornographic photos. Studies consistently show that an elevated P300 occurs when addicts are exposed to cues (such as images) related to their addiction (as in this study on cocaine addicts).
Prause’s often-repeated claim that her subjects “brains did not respond like other addicts” is without support, and nowhere to be found in the actual study. It’s only found in her interviews. Commenting under the Psychology Today interview of Prause, senior psychology professor emeritus John A. Johnson called Prause out for misrepresenting her findings:
“My mind still boggles at the Prause claim that her subjects’ brains did not respond to sexual images like drug addicts’ brains respond to their drug, given that she reports higher P300 readings for the sexual images. Just like addicts who show P300 spikes when presented with their drug of choice. How could she draw a conclusion that is the opposite of the actual results?”
In line with the Cambridge University brain scan studies, Steele et al. 2013 also reported greater cue-reactivity to porn correlating with less desire for partnered sex. To put it another way, individuals with greater brain activation to porn would rather masturbate to porn than have sex with a real person. Shockingly, study spokesperson Prause claimed that porn users merely had “high libido,” yet the results of the study say the exact opposite (subjects’ desire for partnered sex dropped in relation to their porn use). Eight peer-reviewed papers explain the truth: Peer-reviewed critiques of Steele et al., 2013. Also see an extensive YBOP critique.
In summary, a frequent porn user can experience higher subjective arousal (cravings) yet also experience erection problems with a partner. Arousal in response to porn is not evidence of “sexual responsiveness” or healthy erectile function with a partner.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #12: Even David Ley thinks your citation is questionable
SLATE EXCERPT: Experimental studies can demonstrate if porn viewing really causes negative relationship effects by including controls. The first large, preregistered experiment found that viewing sexual pictures did not diminish love or desire for the current romantic partner.
First, it’s absurd to claim that “Experimental studies can demonstrate if porn viewing really causes negative relationship effects.” Experiments where college-aged guys view a few Playboy centerfolds (as in the study linked to by the authors) can tell you nothing about the effects of your husband masturbating to hard-core videos clips day after day for years on end. The only relationship studies that can “demonstrate if porn viewing really causes negative relationship effects” are longitudinal studies that control for variables or studies where subjects abstain from porn. To date seven longitudinal relationship studies have been published that reveal the real-life consequences of ongoing porn use. All reported that porn use relates to poorer relationship/sexual outcomes:
- Adolescents’ Exposure to Sexually Explicit Internet Material and Sexual Satisfaction: A Longitudinal Study (2009).
- A Love That Doesn’t Last: Pornography Consumption and Weakened Commitment to One’s Romantic Partner (2012).
- Internet pornography and relationship quality: A longitudinal study of within and between partner effects of adjustment, sexual satisfaction and sexually explicit internet material among newly-weds (2015).
- Till Porn Do Us Part? Longitudinal Effects of Pornography Use on Divorce, (2016).
- Does Viewing Pornography Reduce Marital Quality Over Time? Evidence from Longitudinal Data (2016).
- Are Pornography Users More Likely to Experience A Romantic Breakup? Evidence from Longitudinal Data (2017).
- Pornography Use and Marital Separation: Evidence from Two-Wave Panel Data (2017).
On to the 2017 study Prause/Klein/Kohut linked to, and its easily dismissed results: Does exposure to erotica reduce attraction and love for romantic partners in men? Independent replications of Kenrick, Gutierres, and Goldberg (1989).
The 2017 study attempted to replicate a 1989 study that exposed men and women in committed relationships to erotic images of the opposite sex. The 1989 study found that men who were exposed to the nude Playboy centerfolds rated their partners as less attractive and reported less love for their partner. As the 2017 failed to replicate the 1989 findings, we are told that the 1989 study got it wrong, and that porn use cannot diminish love or desire. Whoa! Not so fast.
The replication “failed” because our cultural environment has become “pornified.” The 2017 researchers didn’t recruit 1989 college students who grew up watching MTV after school. Instead their subjects grew up surfing PornHub for gang bang and orgy video clips.
In 1989 how many college students had seen an X-rated video? Not too many. How many 1989 college students spent every masturbation session, from puberty on, masturbating to multiple hard-core clips in one session? None. The reason for the 2017 results is evident: brief exposure to a still image of a Playboy centerfold is a big yawn compared to what college men in 2017 have been watching for years. Even the authors admitted the generational differences with their first caveat:
1) First, it is important to point out that the original study was published in 1989. At the time, exposure to sexual content may not have been as available, whereas today, exposure to nude images is relatively more pervasive, and thus being exposed to a nude centerfold may not be enough to elicit the contrast effect originally reported. Therefore, the results for the current replication studies may differ from the original study due to differences in exposure, access, and even acceptance of erotica then versus now.
In a rare instance of unbiased prose even David Ley felt compelled to point out the obvious:
It may be that the culture, men, and sexuality have substantially changed since 1989. Few adult men these days haven’t seen pornography or nude women—nudity and graphic sexuality are common in popular media, from Game of Thrones to perfume advertisements, and in many states, women are permitted to go topless. So it’s possible that men in the more recent study have learned to integrate the nudity and sexuality they see in porn and everyday media in a manner which doesn’t affect their attraction or love for their partners. Perhaps the men in the 1989 study had been less exposed to sexuality, nudity, and pornography.
Keep in mind that this experiment doesn’t mean internet porn use hasn’t affected men’s attraction for their lovers. It just means that looking at “centerfolds” has no immediate impact these days. Many men report radical increases in attraction to partners after giving up internet porn. And, of course, there is also the longitudinal evidence cited above demonstrating the deleterious effects of porn viewing on relationships.
Once again, Prause/Klein/Kohut provide a dubious, cherry-picked result in a feeble attempt to counter the preponderance of studies reporting porn use linked to divorce, breakups, and poorer sexual and relationship satisfaction.
Finally, it’s important to note that the authors of the paper linked to are colleagues of Taylor Kohut at the University of Western Ontario. This group of researchers, headed by William Fisher, has been publishing questionable studies, which consistently produce results that on the surface appear to counter the vast literature linking porn use to myriad negative outcomes. Moreover, both Kohut and Fisher played big roles in the defeat of Motion 47 in Canada.
Here are two recent studies from Kohut, Fisher and colleagues at Western Ontario that garnered widespread and misleading headlines:
In their 2017 study, Kohut, Fisher and Campbell appear to have skewed the sample to produce the results they were seeking. Whereas most studies show that a tiny minority of porn users’ female partners use porn, in this study 95% of the women used porn on their own (85% of the women had used porn since the beginning of the relationship). Those rates are higher than in college-aged men, and far higher than in any other porn study! In other words, the researchers appear to have skewed their sample to produce the results they were seeking. Reality: Cross-sectional data from the largest US survey (General Social Survey) reported that only 2.6% of women had visited a “pornographic website” in the last month.
In addition, Kohut’s study asked only “open ended” questions where subjects could ramble on about porn. The researchers read the ramblings and decided, after the fact, what answers were “important” (fit their desired narrative?). In other words, the study did not correlate porn use with any objective, scientific variable assessment of sexual or relationship satisfaction (as did the over 75 studies that show porn use in linked to negative effects on relationships). Everything reported in the paper was included (or excluded) at the unchallenged discretion of the authors.
Taylor Kohut co-authors framed egalitarianism as: Support for (1) Abortion, (2) Feminist identification, (3) Women holding positions of power, (4) Belief that family life suffers when the woman has a full-time job, and oddly enough (5) Holding more negative attitudes toward the traditional family. Secular populations, which tend to be more liberal, have far higher rates of porn use than religious populations. By choosing these criteria and ignoring endless other variables, lead author Kohut and his co-authors knew they would end up with porn users scoring higher on this study’s carefully chosen selection of what constitutes “egalitarianism.” Then the authors chose a title that spun it all. In reality, these findings are contradicted by nearly every other published study. (See this list of over 25 studies linking porn use to sexist attitudes, objectification and less egalitarianism.)
Note: This 2018 presentation exposes the truth behind 5 questionable and misleading studies, including the two studies just discussed: Porn Research: Fact or Fiction?
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #13: Watching porn makes you horny and drinking improves your mood, so there can be no downside to either
SLATE EXCERPT: In other laboratory research, couples who viewed sex films, whether in the same room or apart, expressed more desire to have sex with that current partner.
Another Nicole Prause paper. Viewing porn, becoming horny, and then wanting to get off, is hardly a remarkable finding. This “laboratory finding” tells us nothing about the long-term effects of porn use on relationships (again, over 75 studies – and every study on men – link porn use to less sexual and relationship satisfaction). This experiment is akin to evaluating the effects of alcohol by asking bar patrons if they feel good after their first couple of beers. Does this onetime assessment tell us anything about their mood the next morning or the long-term effects of chronic alcohol use?
Not surprisingly, Dr. Prause omitted the rest of her study’s findings:
Viewing the erotic films also induced greater reports of negative affect, guilt, and anxiety
Negative affect means negative emotions. Prause has resorted to cherry-picking her own results.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #14: In order to protect porn, let’s blame masturbation for all the negative effects linked to porn
SLATE EXCERPT: While one study reported that reducing pornography consumption increased commitment to a partner, no study has yet shown that this was due to the sex films themselves and not some other confounding variable, such as differences in masturbation that resulted from adjusting viewing habits. In our view, there are not yet compelling data to confirm that sexual arousal via sex films always decreases desire for the regular sex partner; certainly, under some conditions, sex films appear to stoke the fire at home.
Actually, the vast preponderance of the evidence demonstrates convincingly that as pornography consumption increases, relationship and sexual satisfaction decline. This isn’t a case of some studies “say yes” and some studies “say no”, as every study on males and porn use (70 studies) links greater porn use to decreased sexual or relationship satisfaction. In fact, a recent study pointed out that for men, porn use that was more frequent than once per month correlated with reduced sexual satisfaction. (For women, the cut off was even lower. Use that was more frequent than “several times per year” was associated with reduced sexual satisfaction.)
Also, the porn-commitment study cited above actually did show that viewing porn was the most likely cause of reduced commitment in those who viewed more porn. It is one of the few studies to ask people to (attempt to) eliminate porn use (for 3 weeks) to compare the effects with a control group. Incidentally some of the same researchers published another study comparing delayed discounting in those who temporarily tried to quit porn as well. They found that the more porn participants viewed the less able they were to defer gratification. The
It’s ironic that sexologists like Klein, Prause and Kohut are so bent on defending porn use that they’re willing to imply that masturbation causes relationship problems! (Prause and colleague Ley have also claimed masturbation causes chronic ED in young men – without a shred of medical or other evidence)
Yet at the same time Prause has long insisted publicly that masturbation is an unqualified benefit. So, which is it? Here these authors point the finger at masturbation as the cause of relationship problems, but they offer no formal evidence supporting their hunch. It seems their claim that “it’s masturbation” is only a convenient red herring whenever actual scientific evidence demonstrates that more porn use correlates problems.
Incidentally, in 2017 scientists actually tested the “masturbation-red herring” theory, and found no support for it. See “Can Pornography be Addictive? An fMRI Study of Men Seeking Treatment for Problematic Pornography Use” Sensitivity to addiction-related cues was related to both porn use and masturbation frequency. This makes sense, as watching porn is neurologically akin to masturbation:
Take the example of pornography. Thinking about ways to gain access to it, or actively searching for it, and perhaps experiencing desire during the process, is considered sexual wanting. Watching selected pornographic material, even without masturbation, can be considered “having sex” when there is genital arousal.
Humanity urgently needs researchers who will use sound science (and neuroscience) to investigate human sexuality and the effects of today’s unique sexual environment. Not propagandists serving up red herrings.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #15: Sorry kids, only one study has correlated “self-identification as a porn addict” with hours of use, religiousness and moral disapproval of porn use
SLATE EXCERPT: Speaking to the heart of the issue, one of the biggest problems for some porn users is shame. Shame about viewing sex films is heaped on the public by the sex-addiction treatment industry (for profit), by the media (for clickbait), and by religious groups (to regulate sexuality). Unfortunately, whether you believe porn viewing is appropriate or not, stigmatizing sex-film viewing may be contributing to the problem. In fact, an increasing number of studies show that many people who identify as “porn addicted” do not actually view sex films more than other people. They simply feel more shame about their behaviors, which is associated with growing up in a religious or sexually restrictive society.
The response to excerpt #15 has been combined with the response to excerpt #19 below, as both deal with a single pornography questionnaire (CPUI-9) and the mythology surrounding it and the studies that employ it.
Note: The core claim in the above excerpt is false as there is only one study that directly correlated self-identification as a porn addict with hours of use, religiousness and moral disapproval of porn use. Its findings contradict the carefully constructed narrative about “perceived addiction” (that “porn addiction is just religious shame/moral disapproval”) – which is grounded in studies employing the flawed instrument called the CPUI-9. In the only direct-correlation study, the strongest correlation with self-perception as an addict was with hours of porn use. Religiousness was irrelevant, and while there was predictably some correlation between self-perception as an addict and moral incongruence regarding porn use, it was roughly half the hours-of-use correlation.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #16: Compulsivity is not synonymous with the “Compulsive Sexual Behavior Disorder” diagnosis in the ICD-11
SLATE EXCERPT: It is very important to note that compulsivity is not an umbrella term that includes addiction. Addiction, compulsivity, and impulsivity are all different models with different patterns of response that require different treatments. For example, addiction models predict withdrawal symptoms, but compulsivity models do not predict withdrawal. Impulsivity models predict a strong aversion to delaying decisions or delaying expected pleasure, whereas compulsivity models predict rigid, methodical perseverance.
Once again Prause/Klein/Kohut attempt a clever sleight of hand. They want you to believe that “compulsivity” is synonymous with the Compulsive Sexual Behavior Disorder diagnosis, and that therefore the ICD-11 intended to prevent healthcare givers from using it to diagnose those with porn and sex addiction. However, these terms are not synonymous, which means we could disregard excerpt #17 and its muddled attempts to confuse the reader.
Yet we want to unpack this excerpt further because addiction-deniers like Prause/Klein/Kohut and their colleagues seem to have a bit of a compulsion themselves. They insist on relabeling problematic porn use as a “compulsion” – thus implying that it can never be an “addiction.”
RE: “compulsivity is not an umbrella term that includes addiction.” Depends on whom you ask, but such a question is irrelevant to the ICD-11 Compulsive Sexual Behavior Disorder diagnosis. The use of “Compulsive” in the new ICD-11 diagnosis isn’t meant to denote the neurological underpinnings of CSBD: “continued repetitive sexual behaviour despite adverse consequences.” Instead “Compulsive,” as used in the ICD-11, is a descriptive term that’s been in use for years, and is often employed interchangeably with “addiction.” (For example a Google scholar search for compulsion + addiction returns 130,000 citations.)
Excerpt #17 preys on general ignorance of a well established fact: The ICD and DSM systems are descriptive, largely atheoretical classification systems. They rely on the presence or absence of specific signs and symptoms to establish diagnoses. In other words, the ICD and DSM stay away from endorsing any particular biological theory underlying a mental disorder, whether for depression, schizophrenia, alcoholism, or CSBD.
Thus, whatever you or your healthcare giver want to call it – “hypersexuality,” “porn addiction,” “sex addiction,” “out-of-control sexual behavior,” “cybersex addiction” – if the behaviors fall within the “Compulsive Sexual Behaviour Disorder” description, the condition can be diagnosed using the ICD-11 CSBD diagnosis.
Incidentally, as the press release of the Society for the Advancement of Sexual Health explained, the Compulsive Sexual Behavior Disorder is under “impulse control disorders” for now but that may change as it did for Gambling Disorder.
For now, the parent category of the new CSBD diagnosis is Impulse Control Disorders, which includes diagnoses such as Pyromania [6C70], Kleptomania [6C71] and Intermittent Explosive Disorder [6C73]. Yet doubts remain about the ideal category. As Yale neuroscientist Marc Potenza MD PhD and Mateusz Gola PhD, researcher at the Polish Academy of Sciences and the University of California San Diego point out, “The current proposal of classifying CSB disorder as an impulse-control disorder is controversial as alternate models have been proposed …There are data suggesting that CSB shares many features with addictions.” 7
It might be worth noting that ICD-11 includes diagnoses of Gambling Disorder under both Disorders Due to Addictive Behaviors and under Impulse Control Disorders. Thus, categorization of disorders need not always be mutually exclusive.5 Classification may also shift with time. Gambling Disorder was originally classified as an impulse disorder in both the DSM-IV and the ICD-10, but based on advances in empirical understanding, Gambling Disorder has been reclassified as a “Substance-Related and Addictive Disorder” (DSM-5) and a “Disorder Due to Addictive Behaviour” (ICD-11). It is possible that this new CSBD diagnosis may follow a similar developmental course as Gambling Disorder has.
While CSBD looks like an addiction and quacks like an addiction, it starts out in the “Impulse Control Disorders” for political reasons. Politics aside, neuroscientists who publish brain studies on CSB subjects strongly believe its rightful home is with other addictions. From the Lancet commentary, Is excessive sexual behaviour an addictive disorder? (2017):
Compulsive sexual behaviour disorder seems to fit well with non-substance addictive disorders proposed for ICD-11, consistent with the narrower term of sex addiction currently proposed for compulsive sexual behaviour disorder on the ICD-11 draft website. We believe that classification of compulsive sexual behaviour disorder as an addictive disorder is consistent with recent data and might benefit clinicians, researchers, and individuals suffering from and personally affected by this disorder.
By the way, even if “Compulsive Sexual Behaviour Disorder” is eventually moved to the “Disorder Due to Addictive Behaviour” section it will still likely be called “Compulsive Sexual Behaviour Disorder.” Again, “compulsivity” is not synonymous with the diagnosis of CSBD.
RE: Addiction, compulsivity, and impulsivity are all different models with different patterns of response that require different treatments.
First, the link goes to a confused paper that proposes a theoretical “sex addiction” model that just happens to mirror normal sexual patterns of feeling horny, doing the deed, and not feeling longer horny. The model:
Specifically, the sexhavior cycle suggests that the cycle of sexual behavior comprises four distinct and sequential stages described as sexual urge, sexual behavior, sexual satiation, and post-sexual satiation.
That’s it. This inspires me to announce my theoretical model of food intake, with four sequential stages: feeling hungry, urge to eat, eating, feeling full and stopping. The journal solicited commentaries on this proposed “sexhavior cycle.” I recommend this one: Separating Models Obscures the Scientific Underpinnings of Sex Addiction as a Disorder.
Second, addiction studies repeatedly report that addiction features elements of both impulsivity and compulsivity. (A Google Scholar search for addiction + impulsivity + compulsivity returns 22,000 citations.) Here are simple definitions of impulsivity and compulsivity:
- Impulsivity: Acting quickly and without adequate thought or planning in response to internal or external stimuli. A predisposition to accept smaller immediate rewards over larger delayed gratification and an inability to stop a behavior toward gratification once it’s set in motion.
- Compulsivity: Refers to repetitive behaviors that are performed according to certain rules or in a stereotypical fashion. These behaviors persevere even in the face of adverse consequences.
Predictably, addiction researchers often characterize addiction as developing from impulsive pleasure-seeking behavior to compulsive repetitive behaviors to avoid discomfort (such as the pain of withdrawal). Thus, addiction comprises a bit of both, along with other elements. So the differences between “models” of impulsivity and compulsivity as they relate to CSBD are anything but cut and dried.
Third, the concern about different treatment requirements for each model is a red herring as the ICD-11 doesn’t endorse any particular treatment for CSBD or any other mental or physical disorder. That’s up to the healthcare practitioner. In his 2018 paper, “Compulsive sexual behavior: A nonjudgmental approach, CSBD workgroup member Jon Grant (the same expert whom Prause/Klein/Kohut misrepresented earlier) covered misdiagnosis, differential diagnosis, co-morbidities and various treatments options related to the new CSBD diagnosis. Incidentally, Grant says that Compulsive Sexual Behavior is also called “sex addiction” in that paper!
“It’s not an addiction, it’s a compulsion.“ This brings us to the ‘compulsion’ versus ‘addiction’ discussion. Addiction and compulsion are both terms that have entered our everyday language. Like many words that are in common use, they may be misused and misunderstood.
In arguing against the concept of behavioral addictions, especially porn addiction, skeptics often claim that pornography addiction is a ‘compulsion’ and not a true ‘addiction’. Some even insist that addiction is “like” Obsessive-Compulsive Disorder (OCD). When further pressed as to how a ‘compulsion to use X’ differs neurologically from an ‘addiction to X’, a common comeback by these uninformed skeptics is that “behavioral addictions are simply a form of OCD.” Not true.
Multiple lines of research demonstrate that addictions differ from OCD in many substantive ways, including neurological differences. This is why the DSM-5 and ICD-11 have separate diagnostic categories for obsessive-compulsive disorders and for addictive disorders. Studies leave little doubt that CSBD is not a type of OCD. In fact, the percentage of CSB individuals with co-occurring OCD is surprisingly small. From Conceptualization and Assessment of Hypersexual Disorder: A Systematic Review of the Literature (2016)
Obsessive-compulsive spectrum disorders have been considered to conceptualize sexual compulsivity (40) because some studies have found individuals with hypersexual behavior are on the obsessive-compulsive disorder (OCD) spectrum. OCD for hypersexual behavior is not consistent with DSM-5 (1) diagnostic understandings of OCD, which exclude from the diagnosis those behaviors from which individuals derive pleasure. Although obsessive thoughts of the OCD type often have sexual content, the associated compulsions performed in response to the obsessions are not carried out for pleasure. Individuals with OCD report feelings of anxiety and disgust rather than sexual desire or arousal when confronted with situations triggering obsessions and compulsions, with the latter being performed only to quell uneasiness the obsessive thoughts arouse. (41)
From this June, 2018 study: Revisiting the Role of Impulsivity and Compulsivity in Problematic Sexual Behaviors:
Few studies have examined associations between compulsivity and hypersexuality. Among males with nonparaphilic hypersexual disorder [CSBD], the lifetime prevalence of obsessive-compulsive disorder—a psychiatric disorder characterized by compulsivity—ranges from 0% to 14%
Obsessiveness—which may be associated with compulsive behavior—in treatment-seeking men with hypersexuality has been found to be elevated relative to a comparison group, but the effect size of this difference was weak. When the association between the level of obsessive-compulsive behavior—assessed by a subscale of the Structured Clinical Interview for DSM-IV (SCID-II) —and the level of hypersexuality was examined among treatment-seeking males with hypersexual disorder, a trend toward a positive, weak association was found. On the basis of the aforementioned results, compulsivity appears to contribute in a relatively small manner to hypersexuality [CSBD].
In one study, general compulsivity was examined in relation to problematic pornography use among men, showing positive but weak associations. When investigated in a more complex model, the relationship between general compulsivity and problematic pornography use was mediated by sexual addiction and Internet addiction, as well as an addiction more generally. Taken together, the associations between compulsivity and hypersexuality and compulsivity and problematic use appear relatively weak.
There is a current debate regarding how best to consider problematic sexual behaviors (such as hypersexuality and problematic pornography use), with competing models proposing classifications as impulse-control disorders, obsessive-compulsive spectrum disorders, or behavioral addictions. Relationships between transdiagnostic features of impulsivity and compulsivity and problematic sexual behaviors should inform such considerations, although both impulsivity and compulsivity have been implicated in addictions.
The finding that impulsivity related moderately to hypersexuality provides support both for the classification of compulsive sexual behavior disorder (as proposed for ICD-11; World Health Organization as an impulse-control disorder or as a behavioral addiction. In considering the other disorders currently being proposed as impulse-control disorders (e.g., intermittent explosive disorder, pyromania, and kleptomania) and the central elements of compulsive sexual behavior disorder and proposed disorders due to addictive behaviors (e.g., gambling and gaming disorders), the classification of compulsive sexual behavior disorder in the latter category appears better supported. (Emphasis supplied)
Finally, all the physiological and neuropsychological studies published on porn users and porn addicts (often denoted as CSB) report findings consistent with the addiction model (as do studies reporting escalation or tolerance).
In 2016 George F. Koob and Nora D. Volkow published their landmark review in The New England Journal of Medicine: Neurobiologic Advances from the Brain Disease Model of Addiction. Koob is the Director of the National Institute on Alcohol Abuse and Alcoholism (NIAAA), and Volkow is the director of the National Institute on Drug Abuse (NIDA). The paper describes the major brain changes involved with both drug and behavioral addictions, while stating in its opening paragraph that sexual behavioral addictions exist:
We conclude that neuroscience continues to support the brain disease model of addiction. Neuroscience research in this area not only offers new opportunities for the prevention and treatment of substance addictions and related behavioral addictions (e.g., to food, sex, and gambling)….
The Volkow & Koob paper outlined four fundamental addiction-related brain changes, which are: 1) Sensitization, 2) Desensitization, 3) Dysfunctional prefrontal circuits (hypofrontality), 4) Malfunctioning stress system. All 4 of these brain changes have been identified among the many physiological and neuropsychological studies listed on this page:
- Studies reporting sensitization (cue-reactivity & cravings) in porn users/sex addicts: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25.
- Studies reporting desensitization or habituation (resulting in tolerance) in porn users/sex addicts: 1, 2, 3, 4, 5, 6, 7, 8.
- The studies reporting poorer executive functioning (hypofrontality) or altered prefrontal activity in porn users/sex addicts: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17.
- Studies indicating a dysfunctional stress system in porn users/sex addicts: 1, 2, 3, 4, 5.
The preponderance of evidence surrounding CSBD fits the addiction model.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #17: Porn users experience both withdrawal and tolerance
SLATE EXCERPT: For example, addiction models predict withdrawal symptoms, but compulsivity models do not predict withdrawal. Impulsivity models predict a strong aversion to delaying decisions or delaying expected pleasure, whereas compulsivity models predict rigid, methodical perseverance.
RE: withdrawal symptoms. The fact is, withdrawal symptoms are not required to diagnose an addiction. First, you will find the language “neither tolerance nor withdrawal is necessary or sufficient for a diagnosis…” in both the DSM-IV-TR and DSM-5. Second, claiming that “real” addictions cause severe life-threatening withdrawal symptoms mistakenly conflates physiological dependence with addiction-related brain changes. An excerpt from this 2015 review of literature provides a more technical explanation (Neuroscience of Internet Pornography Addiction: A Review and Update):
A key point of this stage is that withdrawal is not about the physiological effects from a specific substance. Rather, this model measures withdrawal via a negative affect resulting from the above process. Aversive emotions such as anxiety, depression, dysphoria, and irritability are indicators of withdrawal in this model of addiction [43,45]. Researchers opposed to the idea of behaviors being addictive often overlook or misunderstand this critical distinction, confusing withdrawal with detoxification [46,47].
Neither Prause, Klein, or Kohut has ever published an addiction study, and it shows. In claiming that withdrawal symptoms and tolerance must be present to diagnosis an addiction they make the rookie mistake of confusing physical dependency with addiction. These terms are not synonymous.
For example, millions of individuals take chronically high levels of pharmaceuticals such as opioids for chronic pain, or prednisone for autoimmune conditions. Their brains and tissues have become dependent on them, and immediate cessation of use could cause severe withdrawals symptoms. However they are not necessarily addicted. Addiction involves multiple well-identified brain changes that lead to what we know as the “addiction phenotype”. If the distinction is unclear, I recommend this simple explanation by NIDA:
Addiction—or compulsive drug use despite harmful consequences—is characterized by an inability to stop using a drug; failure to meet work, social, or family obligations; and, sometimes (depending on the drug), tolerance and withdrawal. The latter reflect physical dependence in which the body adapts to the drug, requiring more of it to achieve a certain effect (tolerance) and eliciting drug-specific physical or mental symptoms if drug use is abruptly ceased (withdrawal). Physical dependence can happen with the chronic use of many drugs—including many prescription drugs, even if taken as instructed. Thus, physical dependence in and of itself does not constitute addiction, but it often accompanies addiction.
That said, internet porn research and numerous self-reports demonstrate that some porn users experience withdrawal and/or tolerance – which are often characteristic of physical dependency. In fact, ex-porn users regularly report surprisingly severe withdrawal symptoms, which are reminiscent of drug withdrawals: insomnia, anxiety, irritability, mood swings, headaches, restlessness, poor concentration, fatigue, depression, social paralysis and the sudden loss of libido that guys call the ‘flatline’ (apparently unique to porn withdrawal). Another sign of physical dependency reported by porn users is requiring porn to get an erection or to have an orgasm.
Changing the label (CSBD) or “model” (i.e. impulsivity) applied to these users doesn’t alter the very real symptoms they report. (See What does withdrawal from porn addiction look like? and this PDF with reports of “withdrawal symptoms.”
Empirical support? Every study that aksed, reported withdrawal symptoms: 10 studies reporting withdrawal symptoms in porn users. For example, consider this graph from a 2017 study reporting the development and testing of a problematic porn use questionnaire. Note that substantial evidence of both “tolerance” and “withdrawal” was found in at-risk users and low-risk users.

A 2018 paper that reported on The Development and Validation of the Bergen-Yale Sex Addiction Scale With a Large National Sample also assessed withdrawal and tolerance. The most prevalent “sex addiction” components seen in the subjects were salience/craving and tolerance, but the other components, including withdrawal, also showed up. Additional studies reporting evidence of withdrawal or tolerance are collected here.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #18: A “Business Insider” article is all you have to support your core assertion?
SLATE EXCERPT: “Sex addiction” was specifically excluded from the ICD-11 for insufficient evidence. This decision is consistent with the opinions of six professional organizations with clinical and research expertise, which also found insufficient evidence to support the idea that sex or porn is addictive.
Regarding the assertion that, “Sex addiction” was specifically excluded from the ICD-11 for insufficient evidence, actually, no, it wasn’t. As explained elsewhere, neither the ICD-11 nor the APA’s DSM-5 ever uses the word “addiction” to describe an addiction – whether it be gambling addiction, or heroin addiction. Both diagnostic manuals title such diagnoses as “disorders” instead. (Details about the peculiar last-minute exclusion of “Hypersexual Disorder” from the DSM-5 are found above under Excerpt #1.) Thus, “sex addiction” was never formally considered for inclusion in either manual (and consequently never “rejected” either).
As for the first link, it goes to a short Business Insider article, not to an official WHO statement. That’s right. Popular media is all the Slate article offers to support the authors’ wishful thinking. Even so, Prause/Klein/Kohut should have read the article before relying on it, as the only scientist quoted states that sexual behavior addictions exist:
Endocrinologist Robert Lustig told Business Insider earlier this year that many activities that can bring feelings of pleasure, like shopping, eating, playing video games, using porn, and even using social media all have addictive potential when taken to extremes. “It does the same thing to your central nervous system as all those drugs do,” he said. “It just doesn’t do the peripheral nervous system part. That doesn’t make it not addiction. It’s still addiction, it’s just that it’s addiction without the peripheral effects.”
Why didn’t the Slate article link to a scientific journal, such as this 2017 Lancet commentary, co-authored by CSBD work-group member Shane Kraus, Ph.D? Well, because the Lancet commentary says the empirical evidence supports CSBD being classified as an addictive disorder:
We believe that classification of compulsive sexual behaviour disorder as an addictive disorder is consistent with recent data and might benefit clinicians, researchers, and individuals suffering from and personally affected by this disorder.
The ICD-11’s Compulsive Sexual Behavior Disorder diagnosis is under “impulse control disorders” for now, but that may change in the future, just as it did for Gambling Disorder. In this responsible article quoting WHO representatives, Kraus leaves open the possibility that CSBD will eventually be placed in the “Disorders Due to Addictive Behaviour” section of the World Health Organization’s diagnostic manual.
And as Kraus puts it, “This is definitely not the final solution, but it’s a good starting place for more research and treatment for people.”
Whatever you or your healthcare giver want to call it – “hypersexuality,” “porn addiction,” “sex addiction,” “out-of-control sexual behavior,” “cybersex addiction” – if the behaviors fall within the “Compulsive Sexual Behaviour Disorder” description, the condition can be diagnosed using ICD-11 the CSBD code.
Re: “six professional organizations.” Actually, the Slate article provided 3 links to “professional organizations” and one link to a 2012 David Ley blog post about the DSM-5 omitting Hypersexual Disorder (which was discussed under excerpt #1). Let’s take a closer look at this impressive-sounding support.
Link #1: Link goes to the infamous 2016 AASECT proclamation. AASECT is not a scientific organization and cited nothing to support the assertions in its own press release – rendering its opinion meaningless.
Most importantly AASECT’s proclamation was pushed through by Michael Aaron and a few other AASECT members using unethical “guerrilla tactics” as Aaron admitted in this Psychology Today blog post: Analysis: How the AASECT Sex Addiction Statement Was Created. An excerpt from this analysis Decoding AASECT’s “Position on Sex Addiction, summarizes Aaron’s blog post:
Finding AASECT’s tolerance of the “sex addiction model” to be “deeply hypocritical,” in 2014 Dr. Aaron set out to eradicate support for the concept of “sex addiction” from AASECT’s ranks. To accomplish his goal, Dr. Aaron claims to have deliberately sowed controversy among AASECT members in order to expose those with viewpoints that disagreed with his own, and then to have explicitly silenced those viewpoints while steering the organization toward its rejection of the “sex addiction model.” Dr. Aaron justified using these “renegade, guerilla [sic] tactics” by reasoning that he was up against a “lucrative industry” of adherents to the “sex addiction model” whose financial incentives would prevent him from bringing them over to his side with logic and reason. Instead, to effect a “quick change” in AASECT’s “messaging,” he sought to ensure that pro-sex addiction voices were not materially included in the discussion of AASECT’s course change.
Dr. Aaron’s boast comes across as a little unseemly. People rarely take pride in, much less publicize, suppressing academic and scientific debate. And it seems odd that Dr. Aaron spent the time and money to become CST certified by an organization he deemed “deeply hypocritical” barely a year after joining it (if not before). If anything, it is Dr. Aaron who appears hypocritical when he criticizes pro-“sex addiction” therapists for having a financial investment in the “sex addiction model”, when, quite obviously, he has a similar investment in promoting his opposing viewpoint
Several commentaries and critiques expose AASECT’s proclamation for what it truly is: sexual politics:
- Alternative Facts: AASECT and the Anti Sex Addiction Rant
- Response to AASECT Position Statement
- Denial of Sex Addiction Hurts Our Clients
- Here’s to Hope for a Change
- How does the AASECT discounting of Sex & Porn Addiction affect the 12-step community?
- The sex addiction debate
Link #2: Link goes to a statement by the Association for the Treatment of Sexual Abusers (ATSA). Nowhere does the position statement suggest that sex addiction does not exist. Instead ATSA reminds us that non-consensual sexual activity is sexual abuse (e.g., Harvey Weinstein) and “likely … not the result of sexual addiction.” Absolutely true.
Link #3: Link goes to a November, 2017 position statement by three non-profit kink organizations. The ‘evidence” they cited was summarily dismantled line by line in the following critique: Dismantling the “group position” paper opposing porn and sex addiction (November, 2017).
Incidentally, it appears that both AASECT and the 3 kink organizations produced their proclamations in a desperate effort to stop the new “CSBD” diagnosis from going into the ICD-11. Evidently, the experts at the World Health Organization were not taken in by this jointly created paper tiger, as the new diagnosis appears in the implementation version of the ICD-11.
Link #4: Link goes to Sex Addiction: Rejected Yet Again by APA. Hypersexual Disorder Will NOT be Included in the DSM5. This David Ley post is noteworthy because it exemplifies the circular tactic employed throughout the Slate article by Ley’s close allies. When the DSM-5 rejected the umbrella diagnosis of “Hypersexual Disorder” Ley and his chums painted it as rejection of “Sex Addiction.” Yet when the ICD-11 included the umbrella diagnosis of “Compulsive Sexual Behavior Disorder” they painted it as excluding “Sex Addiction.” Why worry about internal inconsistencies, right? Just say black is white, and repeat in tweets, on listserves and Facebook and articles like this one by Klein/Kohut/Prause.
Next, back your spin up using an expensive PR firm. It can get you and your propaganda placed in dozens of different mainstream media outlets, touting you as world experts. It matters not if you aren’t an academic, haven’t been affiliated with a university for years, or obtained your PhD from an unaccredited sexology institution.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPTS #15 & #19: The only study to correlate “self-identification as a porn addict” with hours of use, religiousness and moral disapproval found that porn use was by far the best predictor of believing you are addicted to pornography
SLATE EXCERPT: Speaking to the heart of the issue, one of the biggest problems for some porn users is shame. Shame about viewing sex films is heaped on the public by the sex-addiction treatment industry (for profit), by the media (for clickbait), and by religious groups (to regulate sexuality). Unfortunately, whether you believe porn viewing is appropriate or not, stigmatizing sex-film viewing may be contributing to the problem. In fact, an increasing number of studies show that many people who identify as “porn addicted” do not actually view sex films more than other people. They simply feel more shame about their behaviors, which is associated with growing up in a religious or sexually restrictive society.
SLATE EXCERPT: The decision to include sexual compulsivity in ICD-11 strikes us as odd because the exact diagnostic criteria that were chosen have never been tested. Specifically, the ICD-11 asserts that anyone distressed about their frequent sexual behaviors due purely to “moral judgments and disapproval about sexual impulses, urges, or behaviours” should be excluded from diagnosis. However, moral judgments and disapproval are the strongest predictors of someone believing that they are addicted to pornography in the first place.
The following is a combined response to excerpts 15 and 19 as both deal with a single pornography questionnaire (CPUI-9) and the studies that employ it.
Note: The core claim put forth in both excerpts is false as there is only one study that directly correlated self-identification as a porn addict with hours of use, religiousness and moral disapproval of porn use. Its findings contradict the carefully constructed narrative about “perceived addiction” (that “porn addiction is just religious shame/moral disapproval”) – which is grounded in studies employing the
flawed instrument called the CPUI-9. In the only direct-correlation study, the strongest correlation with self-perception as an addict was with hours of porn use. Religiousness was irrelevant, and while there was predictably some correlation between self-perception as an addict and moral incongruence regarding porn use, it was roughly half the hours-of-use correlation.
Here we present a relatively short synopsis of the Joshua Grubbs questionnaire (CPUI-9), the myth of “perceived pornography addiction,” and what the relevant data actually reveal. Since this involves a complex and tangled web with many layers, these three articles and a presentation were produced to fully explain the CPUI-9 studies:
- Is Joshua Grubbs pulling the wool over our eyes with his “perceived porn addiction” research? (2016)
- Religious people use less porn and are no more likely to believe they are addicted (2017)
- YouTube presentation exposing the CPUI-9 and the myth of “perceived addiction”: Pornography Addiction and Perceived Addiction
- New study invalidates the Grubbs CPUI-9 as an instrument to assess either “perceived pornography addiction” or actual pornography addiction (2017)
To understand how the only direct-correlation research undermines all of the CPUI-9 studies, more background is helpful. The phrase “perceived pornography addiction” indicates nothing more than a number: the total score on the following 9-item pornography-use questionnaire with its three extraneous questions. The key insight is that the CPUI-9 includes 3 “guilt and shame/emotional distress” questions not normally found in addiction instruments. These skew its results, causing religious porn users to score higher and non-religious users to score lower than subjects do on standard addiction-assessment instruments. It doesn’t sort the wheat from the chaff in terms of perceived vs. genuine addiction. Nor does the CPUI-9 assess actual porn addiction accurately.
Perceived Compulsivity Section
- I believe I am addicted to Internet pornography.
- I feel unable to stop my use of online pornography.
- Even when I do not want to view pornography online, I feel drawn to it
Access Efforts Section
- At times, I try to arrange my schedule so that I will be able to be alone in order to view pornography.
- I have refused to go out with friends or attend certain social functions to have the opportunity to view pornography.
- I have put off important priorities to view pornography.
Emotional Distress Section
- I feel ashamed after viewing pornography online.
- I feel depressed after viewing pornography online.
- [And] I feel sick after viewing pornography online.
Subjects never “label themselves as porn addicts” in any Grubbs study: They simply answer the 9 questions above, and earn a total score.
The term “perceived pornography addiction” is misleading in the extreme, because it’s just a meaningless score on an instrument that produces skewed results. But people have assumed they understood what “perceived addiction” meant. They presumed it meant that the CPUI-9’s creator, Grubbs, had figured out a way to distinguish actual “addiction” from “belief in addiction.” He hadn’t. He had just given a deceptive label to his “porn use inventory,” the CPUI-9. Grubbs has made no effort to correct the misperceptions about his work that rolled out into the media, pushed by anti-porn addiction sexologists and their media chums.
Misled journalists mistakenly summed up CPUI-9 findings as:
- Believing in porn addiction is the source of your problems, not porn use itself.
- Religious porn users are not really addicted to porn (even if they score high on the Grubbs CPUI-9) – they just have shame.
The Key: the Emotional Distress questions (7-9) cause religious porn users to score much higher and secular porn users to score far lower, as well as creating a strong correlation between “moral disapproval” and total CPUI-9 score (“perceived addiction”). To put it another way, if you use only results from CPUI-9 questions 1-6 (which assess the signs and symptoms of an actual addiction), the correlations dramatically change – and all the dubious articles claiming shame is the “real” cause porn addiction would never have been written.
To look at a few revealing correlations, let’s use data from the 2015 Grubbs paper (“Transgression as Addiction: Religiosity and Moral Disapproval as Predictors of Perceived Addiction to Pornography“). It comprises 3 separate studies and its provocative title suggests that religiosity and moral disapproval “cause” a belief in pornography addiction.
Tips for understanding the numbers in the table: zero means no correlation between two variables; 1.00 means a complete correlation between two variables. The bigger the number the stronger the correlation between the 2 variables.
In this first correlation we see how moral disapproval correlates powerfully with the 3 guilt and shame questions (Emotional Distress), yet weakly with the two other sections that assess actual addiction (questions 1-6). The Emotional Distress questions cause moral disapproval to be the strongest predictor of total CPUI-9 scores (“perceived addiction”).
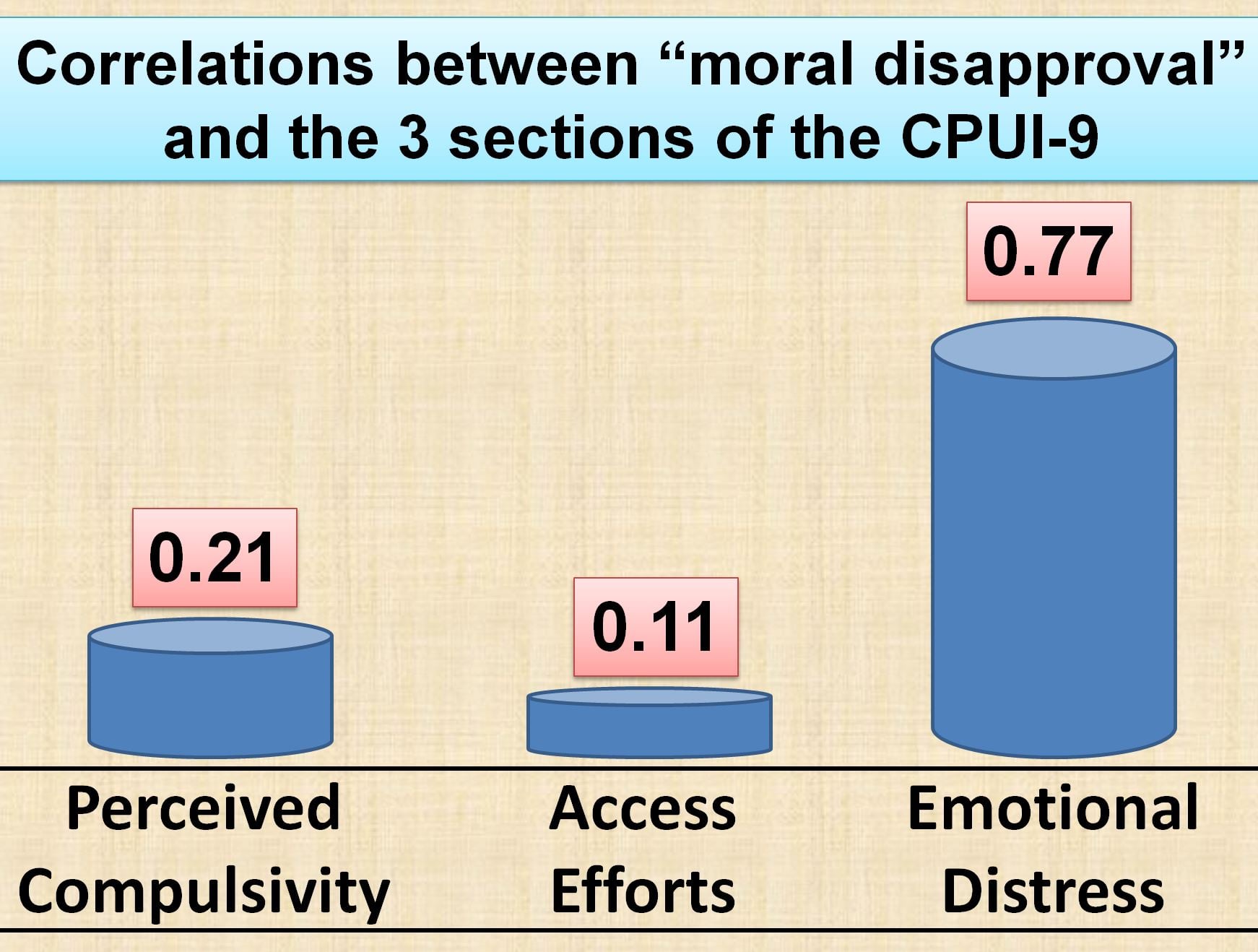
But if we use only the actual porn addiction questions (1-6), the correlation is pretty weak with Moral Disapproval (in science-speak, Moral Disapproval is a weak predictor of porn addiction).
The second half of the story is how the same 3 Emotional Distress correlate very poorly with levels of porn use, while the actual porn addiction questions (1-6) correlate robustly with porn use levels.
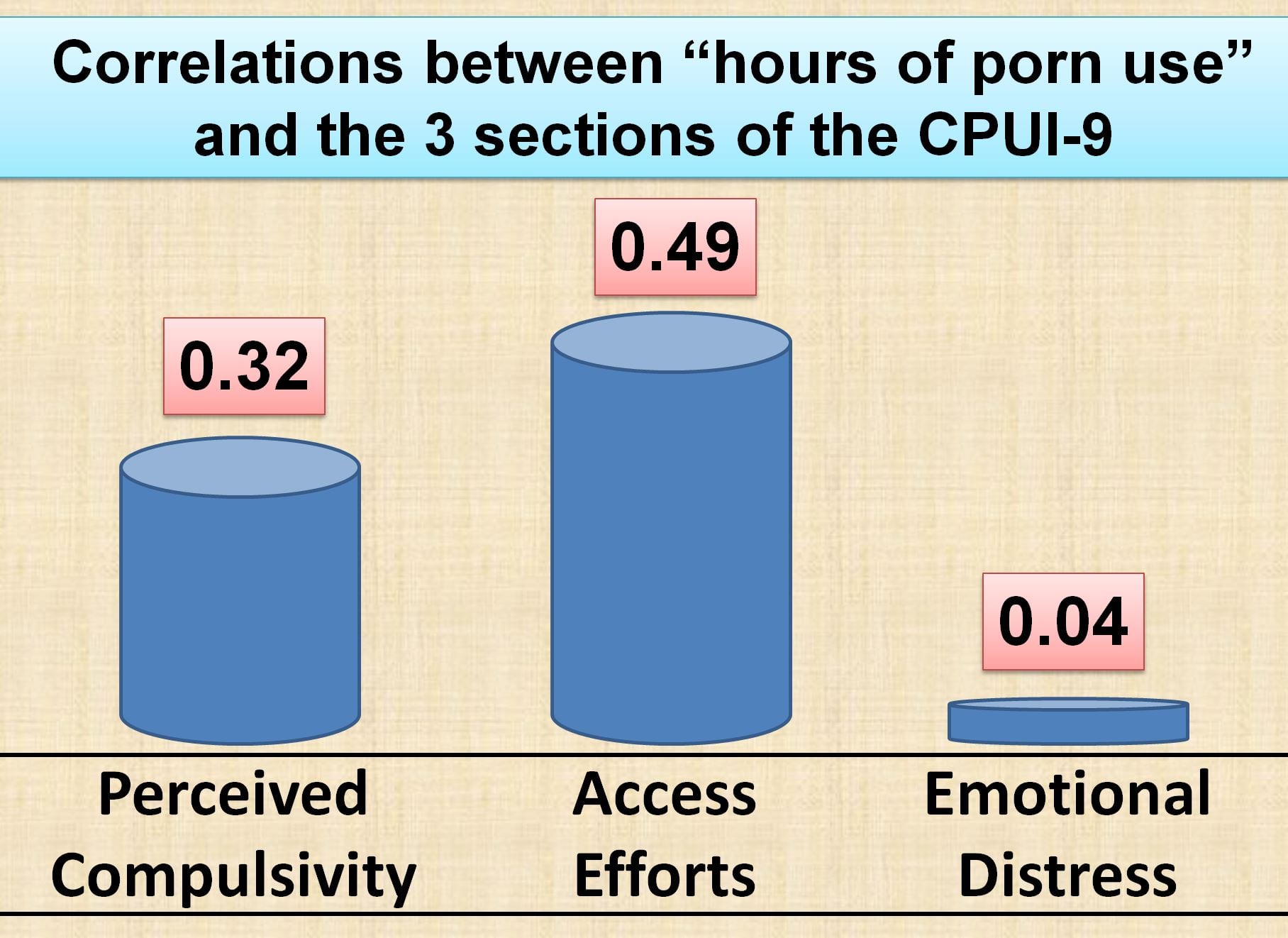
This is how the 3 Emotional Distress questions skew results. They lead to reduced correlations between “hours of porn use” and total CPUI-9 scores (“perceived addiction”). Next, the sum total of all 3 sections of the CPUI-9 test is deceptively re-labeled as “perceived addiction” by Grubbs. Then, at the hands of determined anti-porn-addiction activists, “perceived addiction” morphs into “self identifying as a porn addict.” The activists have pounced on the strong correlation with moral disapproval, which the CPUI-9 always produces, and presto! they now claim that, “a belief in porn addiction is nothing more than shame!”
It’s a house of cards built on 3 guilt and shame question not found in any other addiction assessment, in combination with the misleading term the questionnaire’s creator uses to label his 9 questions (as a measure of “perceived porn addiction”).
The CPUI-9 house of cards came tumbling down with a 2017 study that pretty much invalidates the CPUI-9 as an instrument to assess either “perceived pornography addiction” or actual pornography addiction: Do Cyber Pornography Use Inventory-9 Scores Reflect Actual Compulsivity in Internet Pornography Use? Exploring the Role of Abstinence Effort. It also found that 1/3 of the CPUI-9 questions should be omitted to return valid results related to “moral disapproval,” “religiosity,” and “hours of porn use.” You see all the key excerpts here, but Fernandez et al., 2018 sums things up:
Second, our findings cast doubts on the suitability of the inclusion of the Emotional Distress subscale as part of the CPUI-9. As consistently found across multiple studies (e.g., Grubbs et al., 2015a,c), our findings also showed that frequency of IP use had no relationship with Emotional Distress scores. More importantly, actual compulsivity as conceptualized in the present study (failed abstinence attempts x abstinence effort) had no relationship with Emotional Distress scores.
Emotional Distress scores were significantly predicted by moral disapproval, in line with previous studies which also found a substantial overlap between the two (Grubbs et al., 2015a; Wilt et al., 2016)…. As such, the inclusion of the Emotional Distress subscale as part of the CPUI-9 might skew results in such a way that it inflates the total perceived addiction scores of IP users who morally disapprove of pornography, and deflates the total perceived addiction scores of IP users who have high Perceived Compulsivity scores, but low moral disapproval of pornography.
This may be because the Emotional Distress subscale was based on an original “Guilt” scale which was developed for use particularly with religious populations (Grubbs et al., 2010), and its utility with non-religious populations remains uncertain in light of subsequent findings related to this scale.
Here’s is the core finding: The 3 “Emotional Distress” questions have no place in the CPUI-9, or any porn addiction questionnaire. These guilt and shame questions do not assess distress surrounding addictive porn use or “perception of addiction.” These 3 questions merely artificially inflate total CPUI-9 scores for religious individuals while deflating total CPUI-9 scores for nonreligious porn addicts.
In summary, the conclusions and claims spawned by the CPUI-9 are simply invalid. Joshua Grubbs created a questionnaire that cannot, and was never validated for, sorting “perceived” from actual addiction: the CPUI-9. With zero scientific justification he re-labeled his CPUI-9 as a “perceived pornography addiction” questionnaire.
Because the CPUI-9 included 3 extraneous questions assessing guilt and shame, religious porn users’ CPUI-9 scores tend to be skewed upward. The existence of higher CPUI-9 scores for religious porn users was then fed to the media as a claim that, “religious people falsely believe they are addicted to porn.” This was followed by several studies correlating moral disapproval with CPUI-9 scores. Since religious people as a group score higher on moral disapproval, and (thus) the total CPUI-9, it was pronounced (without actual support) that religious-based moral disapproval is the true cause of pornography addiction. That’s quite a leap, and unjustified as a matter of science.
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
EXCERPT #20: A study accused of using porn stars as its subjects and funded by a controversial for-profit company trying to legitimize its very expensive sexual technique…yeah, that will debunk porn addiction
SLATE EXCERPT: More importantly, we have no laboratory studies about actual sexual behaviors in those who report this difficulty. The first study of partnered sexual behaviors in the laboratory, which tests the compulsivity model, is currently under peer review at a scientific journal. (Disclosure: One of this article’s co-authors, Nicole Prause, is the lead author of that study.) The World Health Organization should wait to see if any science supports their novel diagnosis before risking pathologizing millions of healthy people.
“We have no laboratory studies?” Not so. There are plenty of laboratory studies published on porn’s immediate effects on the viewer (listed in Excerpt #9). More importantly, there are 50 “laboratory studies” assessing brain functions and structures in porn users and those with CSB.
We also have hundreds of studies on adults linking real-life porn use to various negative outcomes such as lower relationship satisfaction, lower sexual satisfaction, divorce, marital separation, relationship breakups, lower levels of commitment, more negative communication, less sex, erectile dysfunctions, anorgasmia, low libido, delayed ejaculation, poorer concentration, poorer working memory, loneliness, depression, anxiety, interpersonal sensitivity, depression, paranoid thinking, psychoticism, addiction, narcissism, reduced happiness, difficulties in intimacy, less relationship trust, devaluation of sexual communication and romantic attachment anxiety.
Similarly, the studies also link real-life porn use to negative body attitude, greater dissatisfaction with muscularity, body fat and height, greater stress, more sexual concerns, less enjoyment of intimate behaviors, increased sexual boredom, less positive communication for both partners, diminished view of women’s competence/morality/humanity, loss of compassion toward women as rape victims, greater belief that women are sex objects, less progressive gender role attitudes, more hostile sexism, opposition to affirmative action, callousness toward sexual violence, thinking of women as entities that exist for men’s sexual gratification, higher adherence to belief that power over women is desirable, lower responsivity to “vanilla sex” erotica, an increased need for novelty and variety…. and a whole lot more.
We have over 270 studies on adolescents reporting that porn use is related to such factors as poorer academics, more sexist attitudes, more aggression, poorer health, poorer relationships, lower life satisfaction, viewing people as objects, increased sexual risk taking, less condom use, greater sexual violence, unexplained anxiety, greater sexual coercion, less sexual satisfaction, lower libido, greater permissive attitudes, social maladjustment, lower self-worth, lower health status, sexually aggressive behavior, addiction, greater gender role conflict, more avoidant and anxious attachment styles, antisocial behaviours, heavy drinking, fighting, ADHD symptoms, cognitive deficits, greater acceptance of pre- and extramarital sex, lower evaluation of marriage, promotion of the acceptance of male dominance and female servitude, less gender egalitarianism, more likely to believe rape myths and prostitution myth…. and a whole lot more.
Will Prause’s upcoming “laboratory study” negate hundreds of studies performed over the last few decades? Highly unlikely as we already know a great deal about her upcoming research on “partnered sexual behaviors.” Both Prause and the lucrative commercial enterprise that funded this research have been crowing about it for years.
What will the partners be doing in the lab? Will the couple be watching porn? Nope. Will the study have a group of carefully screened porn addicts and a control group for comparison? Nope. These are important questions, because Prause’s most famous EEG study suffered from several fatal methodological flaws: 1) subjects were heterogeneous (males, females, non-heterosexuals); 2) subjects were not screened for mental disorders or addictions; 3) study had no control group for comparison; 4) questionnaires were not validated for porn use or porn addiction. 5) Many of the study’s so-called porn addicts really weren’t really porn addicts. Despite this Prause misrepresented her study’s findings, as psychology professor John A. Johnson exposes in two separate comments under a Nicole Prause interview on Psychology Today (comment #1, comment #2 {https://www.psychologytoday.com/us/comment/542939#comment-542939}).
In fact, all existing indications are that her partnered subjects will not be doing anything relevant to this article by Prause/Kohut/Klein. Here’s what we know about this as yet unpublished work: Prause was commissioned by the California company that her website lists as her major source of income, Orgasmic Meditation (also called ‘OM’ and ‘OneTaste’), to study the benefits of clitoral stroking. From Prause’s Liberos website:
Neurological effects and health benefits of orgasmic meditation” Principal Investigator, Direct costs: $350,000, Duration: 2 years, OneTaste Foundation, co-Investigators: Greg Siegle, Ph.D.
OneTaste charges high fees to attend workshops where participants learn “orgasmic meditation” (how to stroke women’s clitorises). This enterprise has recently received some unflattering, revealing publicity (and is now being investigated by the FBI). Here are the news items:
- Shorter, SF Chronicle article – Report alleges ‘sexual servitude’ at San Francisco-based ‘orgasmic meditation’ company
- Longer, investigative article in Bloomberg – The Dark Side of the Orgasmic Meditation Company
The OM/OneTaste company plans to use Prause’s upcoming studies to “scale” their marketing up to new heights. According to the Bloomberg article The Dark Side of the Orgasmic Meditation Company,
The newish CEO is betting that the study OneTaste has funded on the health benefits of OM, which has taken brain-activity readings from 130 pairs of strokers and strokees, will draw fresh crowds. Led by researchers from the University of Pittsburgh, the study is expected to yield the first of multiple papers later this year. “The science that’s coming out to back what this is and what the benefits are is going to be huge in terms of scaling,” Van Vleck says
Regardless of the fact that Prause’s OM research business is addressing partnered clitoral stroking, she is already hinting (as here) or openly claiming (elsewhere) that it invalidates the ICD-11’s new “Compulsive sexual behavior disorder” (CSBD) diagnosis. (Much as her diametrically opposed results in her 2013 and 2015 studies both somehow debunked sex addiction.) In short, whatever research this scientist is hired to perform, you can bet she will claim it debunks porn and sex addiction, as well as the new CSBD that will be used to diagnose both!
Incidentally, where did Prause obtain subjects for her clitoral-stroking investigation? According to tweets by an adult performer, Prause obtained porn performers as OM study subjects, via the most powerful lobbying arm of the porn industry, the Free Speech Coalition. See this Twitter exchange between Prause and adult performer, Ruby the Big Rubousky, who is vice president of the Adult Performers Actors Guild (Prause has since deleted this thread)
Prause responds to Ruby’s tweet is which says one can become addicted to porn

The conversation continues:

Prause has been quick to accuse others of bias without supplying any hard evidence whatsoever, but her OM research is a powerful example of an egregious conflict of interest: taking hundreds of thousands of dollars to find benefits of a dubious, commercially driven practice…and possibly obtaining subjects via the most powerful lobbying arm of the porn industry. All while conveniently serving the porn industry by also claiming this research invalidates the new CSBD diagnosis that will be used for those suffering from compulsive sexual behaviors (more than 80% of whom report problems with internet pornography use).
In another OM-related conflict of interest, Prause and OneTaste CEO Nicole Daedone charged up to $1,900 per person for a 3-day workshop called “Flow & Orgasm.” Like Prause, Nicole Daedone has a long history of questionable behavior. An excerpt from the article The Dark Side of the Orgasmic Meditation Company painted a troublesome picture:
In its 2009 profile, the Times cited former members saying Daedone, the former CEO of OneTaste, possessed “cultlike powers over her followers” and “sometimes strongly suggested who should pair off with whom romantically.”
The workshop for yuppies might be classified as a double-dipping conflict of interest for Dr. Prause: She is first paid several hundred thousand to “prove” the countless benefits of Orgasmic Meditation, then she is paid again for presenting her earth-shaking OM findings at an expensive new-age retreat with the OneTaste CEO that had already paid her to legitimize OM. The circle of life.
A great gig for Prause. However, this calls into question the legitimacy of any reported finding arising from Prause’s OM studies. We have to ask: How can Prause’s OM studies not be biased? This situation is no different from Eli Lilly paying a researcher to “study” the benefits of Prozac, then paying that same researcher big bucks to present about Prozac at medical conferences.
One thought on “Debunking “Why Are We Still So Worried About Watching Porn?” (by Marty Klein, Taylor Kohut, and Nicole Prause)”
Comments are closed.