Introduction
Nicole Prause touts yet another of her letters to the editor as “debunking” the existence of sex addiction and porn addiction (“Compulsive sexual behaviour disorder” in the upcoming ICD-11). Yet it does not. This 240-word opinion piece (Prause et al., 2017) cites zero studies to support its claims, providing only a single, easily refuted sentence as its sole “evidence” countering the addiction model.
This Prause-penned letter in Lancet, signed by four allies (Erick Janssen, Janniko Georgiadis, Peter Finn and James Pfaus), was a reply to another short letter: Is excessive sexual behaviour an addictive disorder? (Potenza et. al., 2017), authored by Marc Potenza, Mateusz Gola, Valerie Voon, Ariel Kor and Shane Kraus. (Both are reproduced below in full.)
Incidentally, three of Prause’s four co-signers in Lancet also lent their names to her earlier 2016 Salt Lake Tribune Op-Ed attacking Fight The New Drug and its position on internet porn. That Salt Lake Tribune 600-word Op-Ed was chock full of unsupported assertions calculated to mislead the lay public. And its authors, Prause and friends, failed to support a single claim. The Op-Ed cited only 4 papers – none of which had anything to do with porn addiction, porn’s effects on relationships, or porn-induced sexual problems. Several experts responded with this dismantling of the Prause Op-Ed: Op-Ed: Who exactly is misrepresenting the science on pornography? (2016). Unlike the “neuroscientists” of the initial Op-Ed, the response authors cited several hundred studies and multiple reviews of the literature that supported their statements.
The one PhD in the Lancet effort who is missing from the Salt Lake Tribune Op-Ed (Peter Finn) happened to co-author a 2014 propaganda piece with Prause and David Ley (the author of The Myth of Sex Addiction), entitled The Emperor Has No Clothes: A Review of the ‘Pornography Addiction’ Model (2014). The paper was not a genuine review, and, difficult as it may be to believe, virtually nothing in the Ley/Prause/Finn paper is accurate or supported by the citations within the paper. The following is a very long analysis of the paper which goes line-by-line, citation by citation, exposing the many shenanigans Ley/Prause/Finn incorporated in their “review”: The Emperor Has No Clothes: A Fractured Fairytale Posing As A Review. Its most remarkable aspect is that it omitted any study that either reported negative effects related to porn use or found porn addiction – and yet labelled itself a “review!”
Update (April, 2019): In an attempt to silence YBOP’s criticism, a handful of authors formed a group (including 4 of the 5 authors on Prause et al., 2017 – Nicole Prause, Erick Janssen, Janniko Georgiadis, Peter Finn) to steal YBOP’s trademark and create a bogus mirror site and social media accounts. See this page for details: Aggressive Trademark Infringement Waged by Porn Addiction Deniers (www.realyourbrainonporn.com).
Turning to Prause’s Lancet effort, we should mention that not one of the five Prause et al., 2017 signers has ever published a study involving verified “porn or sex addicts.” Moreover, some who signed Prause’s Lancet letter have histories of feverishly attacking the concept of porn and sex addiction (thus demonstrating stark bias). In contrast, each of the five Potenza et al. 2017 co-authors (who wrote the first letter on this subject in Lancet) has published multiple studies involving subjects with compulsive sexual behavior disorder (including landmark brain studies on porn users and sex addicts). Question: why is someone who has not been employed by an academic institution for several years, and who openly engages in targeted defamation and harassment of those who suggest porn might be addictive, given a perch for her unsupported propaganda? In an almost unprecedented occurrence, 19 critiques of Prause’s questionable studies have been published in the peer-reviewed literature:
- Steele et al., 2013 – paper 1, paper 2, paper 3, paper 4, paper 5, paper 6, paper 7, paper 8
- Prause et al., 2015 – paper 1, paper 2, paper 3, paper 4, paper 5, paper 6, paper 7, paper 8, paper 9, paper 10
- Prause & Pfaus, 2015 – paper 1
Finally, feel free to ignore Prause et al’s disinformation (below) and go directly to the reputable science in this field. Here’s a list of 30 neuroscience-based literature reviews & commentaries on CSBD by some of the top neuroscientists in the world. All support the addiction model. Alternatively, peruse this list of every neuroscience-based study published on porn users and sex addicts (over 50 to date). They provide strong support for the addiction model as their findings mirror the neurological findings reported in substance addiction studies (contrary to the unsupported assertions in Prause et al.). Finally, consider more than 60 studies reporting findings consistent with escalation of porn use (tolerance), habituation to porn, and even withdrawal symptoms. All are signs and symptoms associated with addiction – thus debunking Prause et al.’s false claim that neither tolerance or withdrawal has been reported in peer-reviewed papers.
Here are the respective letters as they appeared in Lancet:
The Potenza letter and the Prause reply
Is excessive sexual behaviour an addictive disorder? (Potenza et al., 2017)
Marc N Potenza, Mateusz Gola, Valerie Voon, Ariel Kor, Shane W Kraus
Published: September, 2017
In their Comment in The Lancet Psychiatry, John B Saunders and colleagues1 aptly described current debates regarding the consideration and classification of gambling and gaming disorders as addictive disorders, which occurred during the generation of DSM-52 and in anticipation of ICD-11.3 Compulsive sexual behaviour disorder is being proposed as an impulse-control disorder for ICD-11.3 However, we believe the logic applied by Saunders and colleagues1 might also apply to compulsive sexual behaviour disorder. Compulsive sexual behaviour disorder (operationalised as hypersexual disorder) was considered for inclusion in DSM-5 but ultimately excluded, despite the generation of formal criteria and field trial testing.2 This exclusion has hindered prevention, research, and treatment efforts, and left clinicians without a formal diagnosis for compulsive sexual behaviour disorder.
Research into the neurobiology of compulsive sexual behaviour disorder has generated findings relating to attentional biases, incentive salience attributions, and brain-based cue reactivity that suggest substantial similarities with addictions.4 Compulsive sexual behaviour disorder is being proposed as an impulse-control disorder in ICD-11, consistent with a proposed view that craving, continued engagement despite adverse consequences, compulsive engagement, and diminished control represent core features of impulse-control disorders.5 This view might have been appropriate for some DSM-IV impulse-control disorders, specifically pathological gambling. However, these elements have long been considered central to addictions, and in the transition from DSM-IV to DSM-5, the category of Impulse Control Disorders Not Elsewhere Classified was restructured, with pathological gambling renamed and reclassified as an addictive disorder.2 At present, the ICD-11 beta draft site lists the impulse-control disorders, and includes compulsive sexual behaviour disorder, pyromania, kleptomania, and intermittent explosive disorder.3
There are both pros and cons regarding the classification of compulsive sexual behaviour disorder as an impulse-control disorder. On one hand, inclusion of compulsive sexual behaviour disorder in ICD-11 could improve consistency in diagnosis, treatment, and study of individuals with this disorder. On the other hand, classification of compulsive sexual behaviour disorder as an impulse-control disorder as opposed to an addictive disorder might negatively influence treatment and study by limiting treatment availability, treatment training, and research efforts. Compulsive sexual behaviour disorder seems to fit well with non-substance addictive disorders proposed for ICD-11, consistent with the narrower term of sex addiction currently proposed for compulsive sexual behaviour disorder on the ICD-11 draft website.3 We believe that classification of compulsive sexual behaviour disorder as an addictive disorder is consistent with recent data and might benefit clinicians, researchers, and individuals suffering from and personally affected by this disorder.
References:
-
- Excessive gambling and gaming: addictive disorders? Lancet Psychiatry. 2017; 4: 433-435 PubMed
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders (DSM-5). American Psychiatric Association Publishing, Arlington; 2013. Google Scholar
- WHO. ICD-11 beta draft. http://apps.who.int/classifications/icd11/browse/l-m/en (accessed July 18, 2017).
- Should compulsive sexual behavior be considered an addiction? Addiction. 2016; 111: 2097-2106 PubMed
- Impulse control disorders and “behavioural addictions” in the ICD-11. World Psychiatry. 2014; 13: 125-127 PubMed
++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++++
Data do not support sex as addictive (Prause et al., 2017)
Nicole Prause, Erick Janssen, Janniko Georgiadis, Peter Finn, James Pfaus
Published: December, 2017
Marc Potenza and colleagues1 advocated classifying “excessive sexual behaviour” as an addictive disorder in ICD-11. Sex has components of liking and wanting that share neural systems with many other motivated behaviours.2 However, experimental studies do not support key elements of addiction such as escalation of use, difficulty regulating urges, negative effects, reward deficiency syndrome, withdrawal syndrome with cessation, tolerance, or enhanced late positive potentials. A key neurobiological feature of addiction is the increased responsiveness of glutamate neurons that synapse on the nucleus accumbens. These changes might affect long-term sensitisation of the mesocorticolimbic dopamine pathway, as manifested by a range of symptoms including cue-induced craving and compulsive drug use. 3 To date, research on the effects of sex on glutamate function and its modulation of dopamine pathways is scarce.
Sex is a primary reward, with unique peripheral representation. Engagement in sex is positively associated with health and life satisfaction. Sex does not allow for supraphysiological stimulation. Research in this area has yet to investigate actual partnered sexual behaviours. Experimental work has been limited to sexual cues, or secondary rewards, using images. More research is needed, but data concerning frequent or excessive sex do not support its inclusion as an addiction. Also, data are not sufficient to differentiate between compulsive and impulsive models. Many other approaches exist, including well-supported non-pathological models.4 Potenza and colleagues5 also stated that addiction criteria were not met for sexual behaviours: we agree with this earlier conclusion.
References:
-
- Is excessive sexual behaviour an addictive disorder? Lancet Psychiatry. 2017; 4: 663-664 PubMed
- Sex for fun: a synthesis of human and animal neurobiology. Nat Rev Urol. 2012; 9: 486-498 PubMed
- Drug addiction as a pathology of staged neuroplasticity. Neuropsychopharmacology. 2008; 33: 166-180 PubMed
- Hypersexuality: a critical review and introduction to the “sexhavior cycle”. Arch Sex Behav. 2017; DOI:10.1007/s10508-017-0991-8<
- Should compulsive sexual behavior be considered an addiction? Addiction. 2016; 111: 2097-2106 PubMed
Debunking the solitary sentence containing everything Prause et al. 2017 had to offer
Prause’s Lancet effort contains only a single sentence (and no supporting citations) to counter the Potenza et al. commentary. (In support of Potenza et al., consider these 25 commentaries/reviews asserting that CSBD should be categorized under the “addictive behaviors” category in WHO’s new ICD-11.) Prause et al. provides seven so-called “key elements of addiction” its authors claim studies have yet to find in porn or sex addicts:
PRAUSE ET AL: However, experimental studies do not support key elements of addiction such as escalation of use, difficulty regulating urges, negative effects, reward deficiency syndrome, withdrawal syndrome with cessation, tolerance, or enhanced late positive potentials.
Reality check:
- Three of Prause’s seven items are not really accepted as “key elements of addiction”: Reward deficiency syndrome, enhanced late positive potentials, and withdrawal. In fact, however, studies have reported both withdrawal and reward deficiency syndrome in porn user and sex addicts. Her other purported key element of addiction (“enhanced late positive potentials”) has only been assessed in a widely criticized Nicole Prause EEG study. Seven peer-reviewed papers agree that Prause’s finding of lower EEG readings (lower late positive potentials) actually means that frequent porn users were bored by vanilla porn (an indication of possible addiction). In fact, these formal analyses of Prause’s paper agree that she found desensitization/habituation in frequent porn users (consistent with the addiction model): 1, 2, 3, 4, 5, 6, 7, 8, 9, 10
- Thus, contrary to Prause’s claims, six of the seven so-called “elements of addiction” have been identified in studies on porn users and/or sex addicts – and the seventh rests solely on her own dubious claim (that it is “key”) and her own disputed analysis.
Readers need to ask themselves why Prause et al. would attempt to mislead them.
Before we provide empirical support for the “key elements of addiction” that Prause et al. claimed were absent, let’s briefly examine what addiction experts believe are actually the key elements of addiction:
The major brain changes induced by addiction are described by George F. Koob and Nora D. Volkow in their landmark review: Neurobiologic Advances from the Brain Disease Model of Addiction (2016). Koob is the Director of the National Institute on Alcohol Abuse and Alcoholism (NIAAA), and Volkow is the director of the National Institute on Drug Abuse (NIDA).
The paper describes four key brain changes involved with both drug and behavioral addictions, and how they manifest behaviorally: 1) Sensitization, 2) Desensitization, 3) Dysfunctional prefrontal circuits (hypofrontality), 4) Malfunctioning stress system. All 4 of these brain changes have been identified among the many neurological studies listed on this page:
- Studies reporting sensitization in porn users/sex addicts: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27.
- Assessed via cue-reactivity brain studies or strong cravings to use.
- Studies reporting desensitization or habituation in porn users/sex addicts: 1, 2, 3, 4, 5, 6, 7, 8. Manifests as decreased reward sensitivity (less pleasure), habituation to porn (lower brain activation), tolerance (escalation to new genres).
- Studies reporting poorer executive functioning (hypofrontality) or altered prefrontal activity in porn users/sex addicts: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19. Manifests as weakened willpower, cravings, inability to control use, poor decision making.
- Studies indicating a dysfunctional stress system in porn users/sex addicts: 1, 2, 3, 4, 5.
- Manifests as even minor stress leading to cravings and relapse because it activates powerful sensitized pathways. In addition, quitting an addiction activates the brain’s stress systems leading to many of the withdrawal symptoms common to all addictions, such as anxiety, irritability and mood swings.
As we can see Prause et al., 2017, cherry-picked and misrepresented key elements of addiction to produce a “official” letter to link to on social media and to email journalists.
Empirical support for the “key elements of addiction” that Prause et al. claimed were absent
In this section we provide empirical support for the “key elements of addiction” that Prause falsely asserted were absent.
PRAUSE ET AL: However, experimental studies do not support key elements of addiction such as escalation of use, difficulty regulating urges, negative effects, reward deficiency syndrome, withdrawal syndrome with cessation, tolerance, or enhanced late positive potentials.
1) “escalation of use” and “tolerance”
Prause et al. incorrectly lists “tolerance” and “escalation of use” as separate elements of addiction. Tolerance, which is the need for greater stimulation in order to achieve the same level of arousal is also called habituation (less and less response to a drug or a stimulus). With drug abusers tolerance/habituation manifests as needing higher doses to achieve the same high. This is escalation of use. With porn users, tolerance/habituation leads to boredom with current genre or type of porn: greater stimulation is often achieved by escalating to new or more extreme genres of porn.
While a tremendous amount of clinical and anecdotal evidence exists for tolerance leading to escalation in porn users, are there any studies? In fact, over 50 studies have reported findings consistent habituation or escalation in frequent porn users – all conveniently ignored by Prause and her biased co-authors. Here we provide a few examples of escalation and habituation/tolerance from this list of 50 studies:
One of the first studies to ask porn users directly about escalation: “Online sexual activities: An exploratory study of problematic and non-problematic usage patterns in a sample of men” (2016). The study reports escalation, as 49% of the men reported viewing porn that was not previously interesting to them or that they once considered disgusting. An excerpt:
Forty-nine percent mentioned at least sometimes searching for sexual content or being involved in OSAs that were not previously interesting to them or that they considered disgusting.
“The Dual Control Model: The Role Of Sexual Inhibition & Excitation In Sexual Arousal And Behavior,” 2007. Indiana University Press, Editor: Erick Janssen, pp.197-222. In an experiment employing video porn (of the type used in previous experiments), 50% of the young men couldn’t become aroused or achieve erections with porn (average age was 29). The shocked researchers discovered that the men’s erectile dysfunction was,
related to high levels of exposure to and experience with sexually explicit materials.
The men experiencing erectile dysfunction had spent a considerable amount of time in bars and bathhouses where porn was “omnipresent,” and “continuously playing.” The researchers stated:
Conversations with the subjects reinforced our idea that in some of them a high exposure to erotica seemed to have resulted in a lower responsivity to “vanilla sex” erotica and an increased need for novelty and variation, in some cases combined with a need for very specific types of stimuli in order to get aroused.
How about a brain scan study? “Brain Structure and Functional Connectivity Associated With Pornography Consumption: The Brain on Porn” (Kühn & Gallinat, 2014). This Max Planck Institute fMRI study found less grey matter in the reward system (dorsal striatum) correlating with the amount of porn consumed. It also found that more porn use correlated with less reward circuit activation while briefly viewing sexual photos. Researchers hypothesized that their findings indicated desensitization, and possibly tolerance, which is the need for greater stimulation to achieve the same level of arousal. Lead author Simone Kühn said the following about her study:
This could mean that regular consumption of pornography dulls the reward system. … We therefore assume that subjects with high pornography consumption require ever stronger stimuli to reach the same reward level …. This is consistent with the findings on the functional connectivity of the striatum to other brain areas: high pornography consumption was found to be associated with diminished communication between the reward area and the prefrontal cortex.
Another brain scan study “Novelty, conditioning and attentional bias to sexual rewards“ (2015). Cambridge University fMRI study reporting greater habituation to sexual stimuli in compulsive porn users. An excerpt:
Online explicit stimuli are vast and expanding, and this feature may promote escalation of use in some individuals. For instance, healthy males viewing repeatedly the same explicit film have been found to habituate to the stimulus and find the explicit stimulus as progressively less sexually arousing, less appetitive and less absorbing (Koukounas and Over, 2000). … We show experimentally what is observed clinically that Compulsive Sexual Behavior is characterized by novelty-seeking, conditioning and habituation to sexual stimuli in males.
From the related press release:
This same habituation effect occurs in healthy males who are repeatedly shown the same porn video. But when they then view a new video, the level of interest and arousal goes back to the original level. This implies that, to prevent habituation, the sex addict would need to seek out a constant supply of new images. In other words, habituation could drive the search for novel images.
“Our findings are particularly relevant in the context of online pornography,” adds Dr Voon. “It’s not clear what triggers sex addiction in the first place and it is likely that some people are more pre-disposed to the addiction than others, but the seemingly endless supply of novel sexual images available online helps feed their addiction, making it more and more difficult to escape.”
How about Prause’s own EEG study, which itself actually found habituation? Modulation of Late Positive Potentials by Sexual Images in Problem Users and Controls Inconsistent with “Porn Addiction” (Prause et al., 2015). Compared to controls “individuals experiencing problems regulating their porn viewing” had lower brain responses to one-second exposure to photos of vanilla porn. The lead author claims these results “debunk porn addiction.” Incidentally, what legitimate scientist would claim that their lone anomalous study has debunked a well established field of study?
In reality, the findings of Prause et al. 2015 align perfectly with Kühn & Gallinat (2014), which found that more porn use correlated with less brain activation in response to pictures of vanilla porn. The Prause et al. findings also align with Banca et al. 2015, which reported that lower EEG readings meant that subjects were paying less attention to the pictures than controls. Put simply, frequent porn users were desensitized to static images of vanilla porn. They were bored (habituated or desensitized). See this extensive YBOP critique. No less than 9 peer-reviewed papers agree that Prause et al. 2015 actually found desensitization/habituation in frequent porn users (which is consistent with addiction): Peer-reviewed critiques of Prause et al., 2015
A study that reported both tolerance and withdrawal (two items Prause’s Lancet piece falsely claimed that no study had reported either): “The Development of the Problematic Pornography Consumption Scale (PPCS)” (2017) – This paper developed and tested a problematic porn use questionnaire that was modeled after substance addiction questionnaires. This 18-item questionnaire assessed tolerance and withdrawal with the following 6 questions:

———-

Each question was scored from one to seven on a Likert scale: 1- Never, 2- Rarely, 3- Occasionally, 4- Sometimes, 5- Often, 6- Very Often, 7- All the Time. The graph below grouped porn users into 3 categories based on their total scores: “Nonproblematic,” “Low risk,” and “At risk.” Results below show that many porn users experience both tolerance and withdrawal
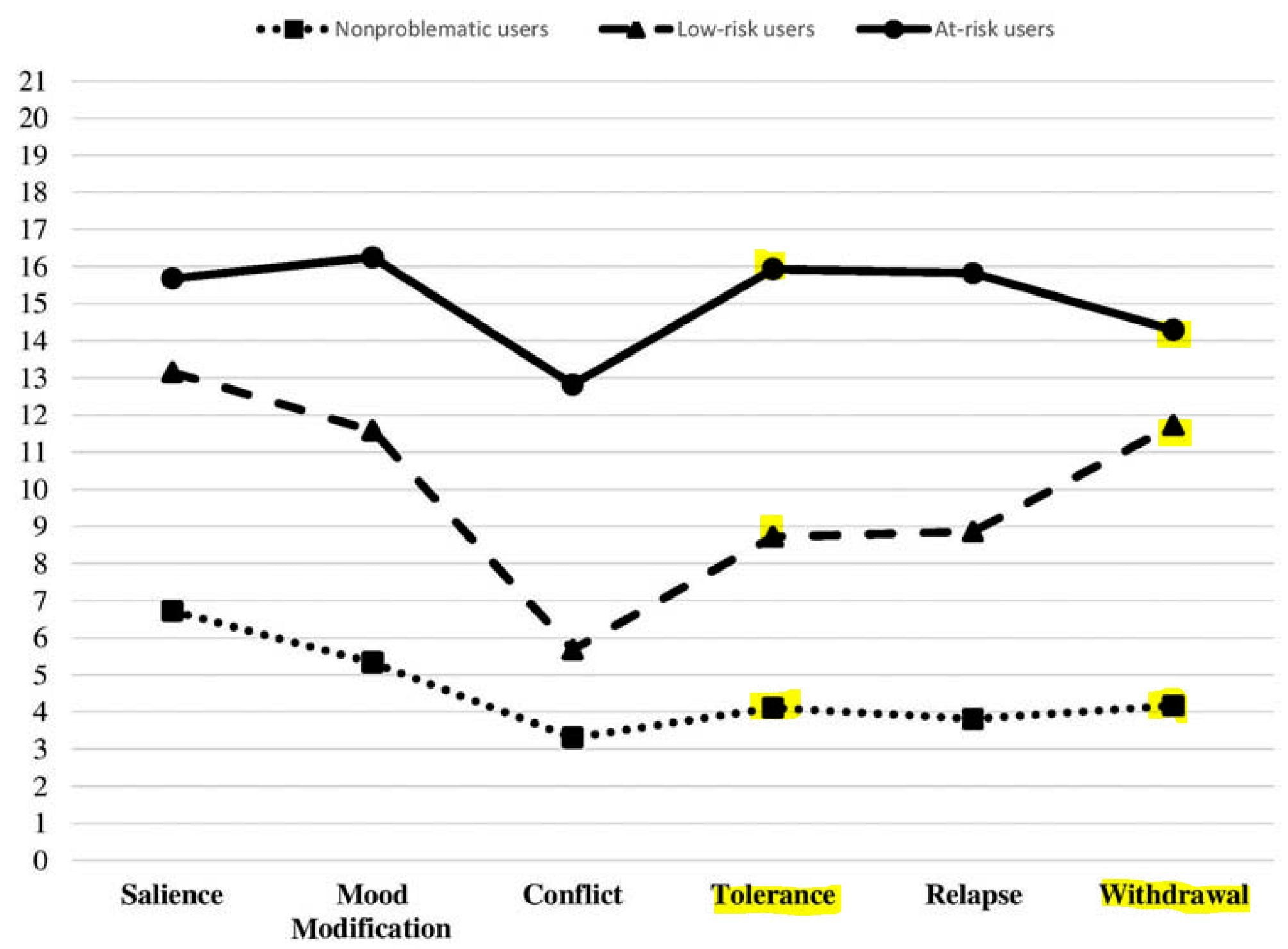
Put simply, this study actually asked about escalation (tolerance) and withdrawal – and both are reported by some porn users.
This very large (n = 6463) study of young people pretty much debunks every Prause et al. assertion – Prevalence, Patterns and Self-Perceived Effects of Pornography Consumption in Polish University Students: A Cross-Sectional Study (2019). It reported everything Prause claims doesn’t exist: tolerance/habituation, escalation of use, needing more extreme genres to be sexually aroused, withdrawal symptoms when quitting, porn-induced sexual problems, porn addiction, and more. A few excerpts related to tolerance/habituation/escalation:
The most common self-perceived adverse effects of pornography use included: the need for longer stimulation (12.0%) and more sexual stimuli (17.6%) to reach orgasm, and a decrease in sexual satisfaction (24.5%)…
The present study also suggests that earlier exposure may be associated with potential desensitization to sexual stimuli as indicated by a need for longer stimulation and more sexual stimuli required to reach orgasm when consuming explicit material, and overall decrease in sexual satisfaction…..
Various changes of pattern of pornography use occurring in the course of the exposure period were reported: switching to a novel genre of explicit material (46.0%), use of materials that do not match sexual orientation (60.9%) and need to use more extreme (violent) material (32.0%). The latter was more frequently reported by females considering themselves as curious compared tothose regarding themselves as uninquisitive
the present study found that a need to use more extreme pornography material was more frequently reported by males describing themselves as aggressive.
Additional signs of tolerance/escalation: needing multiple tabs open and using porn outside of home:
The majority of students admitted to use of private mode (76.5%, n = 3256) and multiple windows (51.5%, n = 2190) when browsing online pornography. Use of porn outside residence was declared by 33.0% (n = 1404).
Earlier age of first use related to greater problems and addiction (this indirectly indicates tolerance-habituation-escalation):
Age of first exposure to explicit material was associated with increased likelihood of negative effects of pornography in young adults—the highest odds were found for females and males exposed at 12 years or below. Although a cross-sectional study does not allow an assessment of causation, this finding may indeed indicate that childhood association with pornographic content may have long-term outcomes….
Addiction rates were relatively high, even though it was “self-perceived”:
Daily use and self-perceived addiction was reported by 10.7% and 15.5%, respectively.
The study reported withdrawal symptoms, even in non-addicts (a definitive sign of addiction-related brain changes):
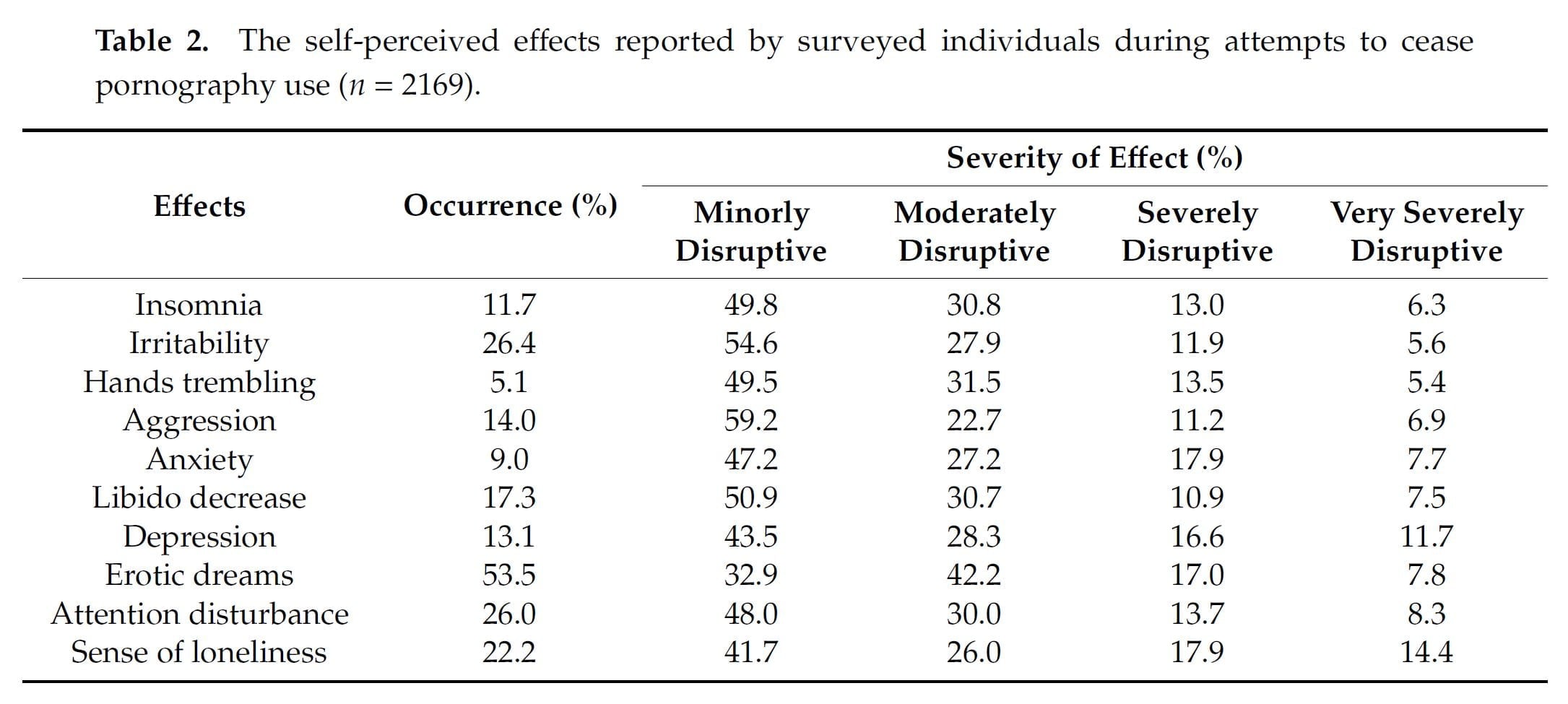
Among those surveyed who declared themselves to be current pornography consumers (n = 4260), 51.0% admitted to making at least one attempt to give up using it with no dif ference in the frequency of these attempts between males and females. 72.2% of those attempting to quit pornography use indicated the experience of at least one associated e ffect, and the most frequently observed included erotic dreams (53.5%), irritability (26.4%), attention disturbance (26.0%), and sense of loneliness (22.2%) (Table 2).
I could provide 45 more studies reporting or suggesting habituation to “regular porn” along with escalation into more extreme and unusual genres, but Prause et al. is already exposed for what it is – propaganda masquerading as a scholarly letter to the editor.
2) “negative effects”
Since hundreds of studies have linked porn/sex addiction and porn use to myriad negative effects, Prause’s Lancet claim that no study has reported negative effects exposes the letter as a scam.
This preposterous claim is debunked by the hundreds of studies examining assessing compulsive sexual behaviour, most of which employed one or more of the following porn/sex addiction instruments. The core element of an addiction is “continued use despite severe negative consequences.” That’s why following questionnaires all asked about negative effects related to CSB (links are to Google scholar studies):
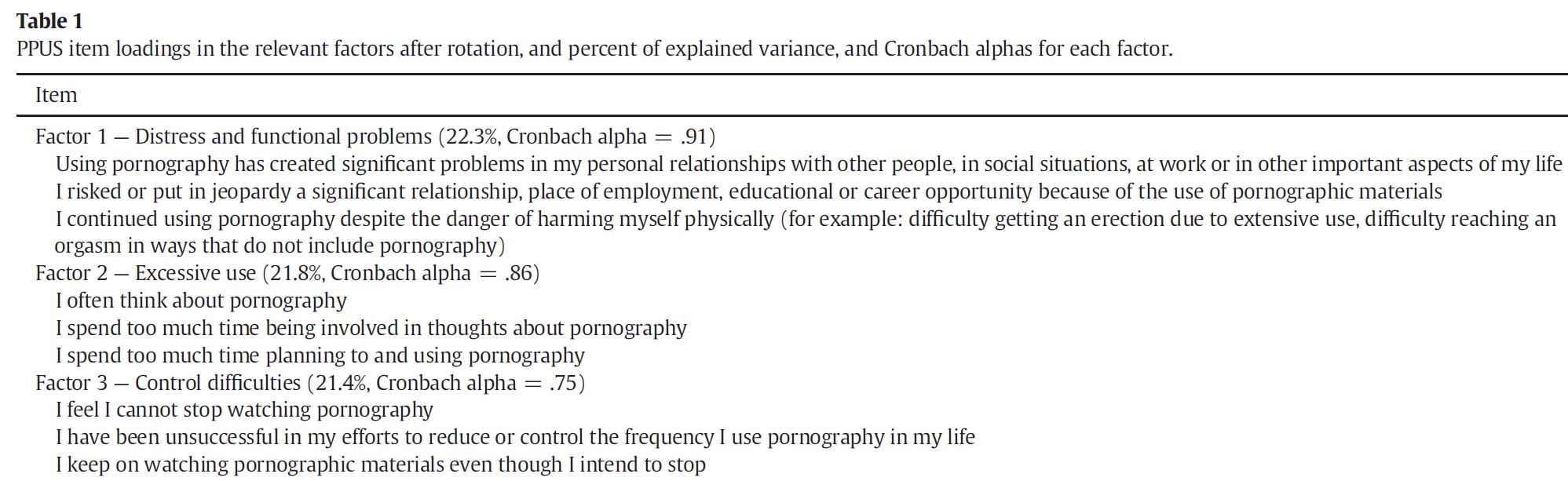
- Problematic Pornography Use Scale (PPUS),
- Compulsive Pornography Consumption (CPC),
- Cyber Pornography Use Inventory (CPUI),
- Cognitive and Behavioral Outcomes Scale (CBOSB),
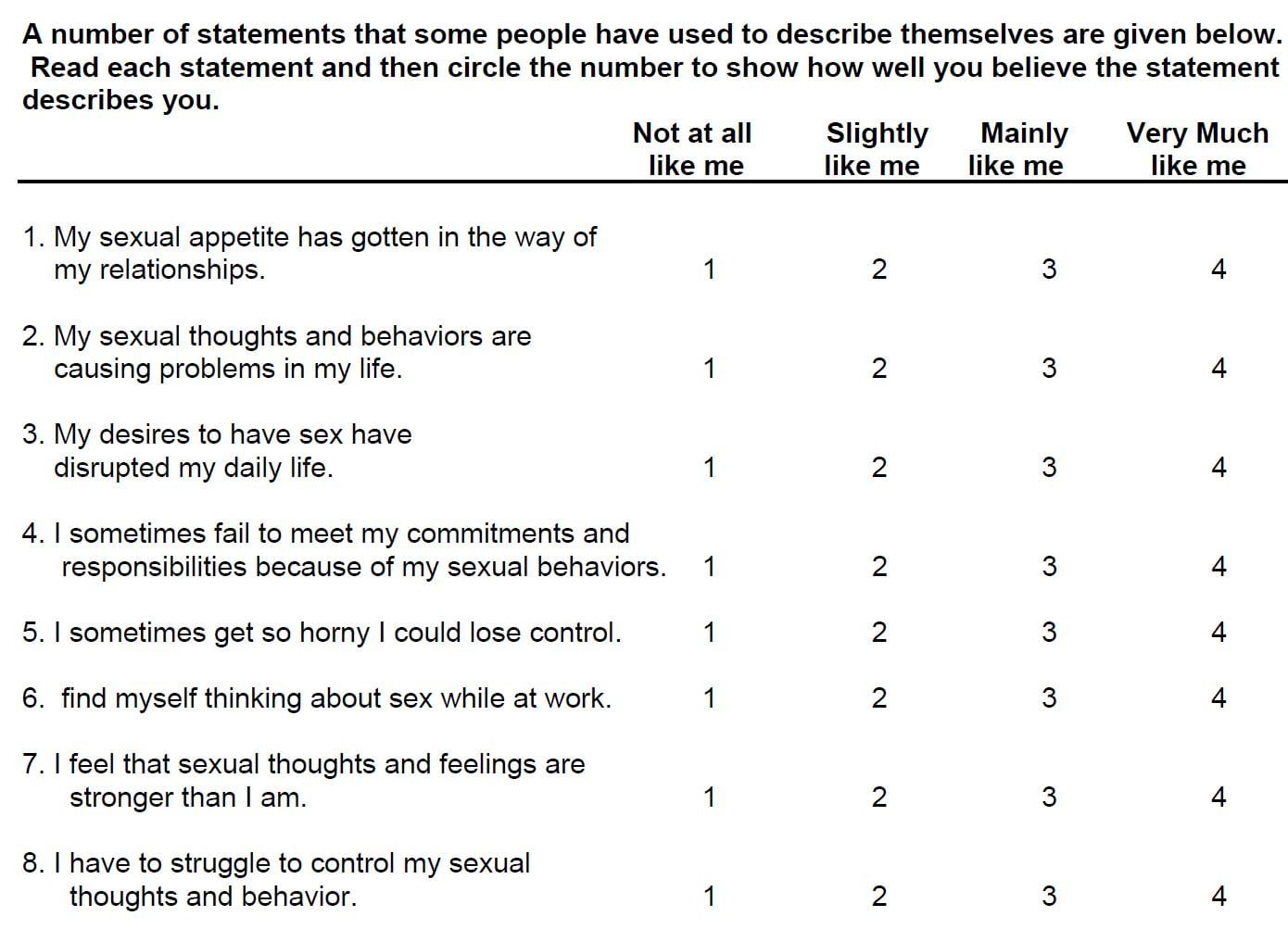
- Sexual Compulsivity Scale (SCS),
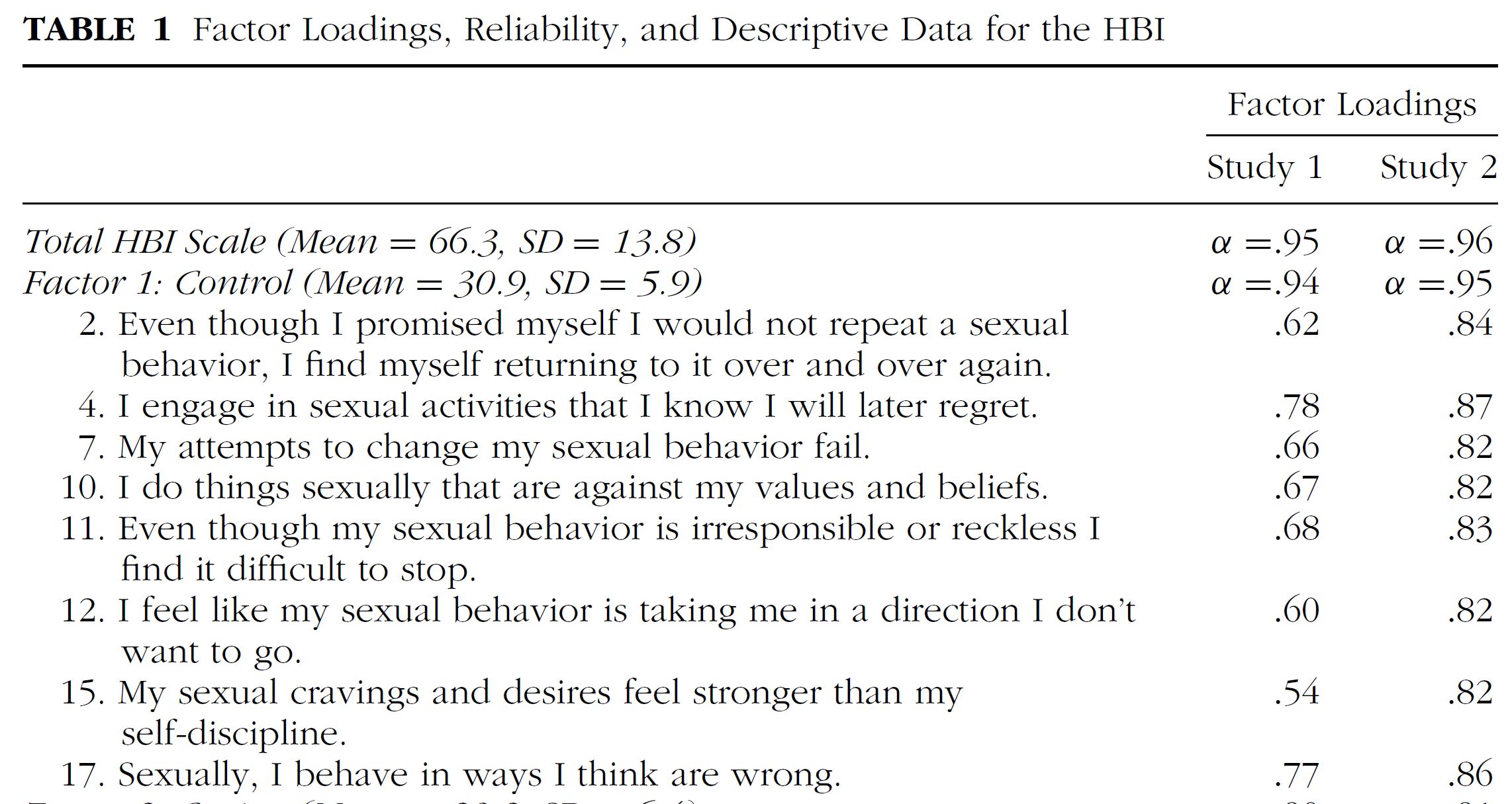
- Hypersexual Behavior Inventory (HBI),
- Pornography Craving Questionnaire (PCQ),
- Hypersexual Behavior Consequences Scale (HBCS)
- Internet Addiction Test-sex (IAT-sex)
- Problematic Pornography Consumption Scale (PPCS)
Even apart from the issue of addiction risk, the preponderance of empirical evidence links porn use to various negative outcomes. For example, over 70 studies link porn use to less sexual and relationship satisfaction. As far as we know all studies involving males have reported that more porn use is linked to poorer sexual or relationship satisfaction. Porn and sexual problems? This list contains 35 studies linking porn use/porn addiction to sexual problems and lower arousal to sexual stimuli.
Porn use affecting emotional and mental health? Over 65 studies link porn use to poorer mental-emotional health & poorer cognitive outcomes.
Porn use affecting beliefs, attitudes and behaviors? Check out individual studies: over 35 studies link porn use to “un-egalitarian attitudes” toward women and sexist views. Or consider this summary from this 2016 meta-analysis – Media and Sexualization: State of Empirical Research, 1995–2015. Excerpt:
A total of 109 publications that contained 135 studies were reviewed. The findings provided consistent evidence that both laboratory exposure and regular, everyday exposure to this content are directly associated with a range of consequences, including higher levels of body dissatisfaction, greater self-objectification, greater support of sexist beliefs and of adversarial sexual beliefs, and greater tolerance of sexual violence toward women. Moreover, experimental exposure to this content leads both women and men to have a diminished view of women’s competence, morality, and humanity.
What about sexual aggression and porn use? Another meta-analysis: A Meta‐Analysis of Pornography Consumption and Actual Acts of Sexual Aggression in General Population Studies (2015). Excerpt:
22 studies from 7 different countries were analyzed. Consumption was associated with sexual aggression in the United States and internationally, among males and females, and in cross-sectional and longitudinal studies. Associations were stronger for verbal than physical sexual aggression, although both were significant. The general pattern of results suggested that violent content may be an exacerbating factor.
What about the porn use and adolescents? Check out this list of over 250 adolescent studies, or these reviews of the literature: review#1, review2, review#3, review#4, review#5, review#6, review#7, review#8, review#9, review#10, review#11, review#12, review#13. From the conclusion of this 2012 review of the research – The Impact of Internet Pornography on Adolescents: A Review of the Research:
Collectively, these studies suggest that youth who consume pornography may develop unrealistic sexual values and beliefs. Among the findings, higher levels of permissive sexual attitudes, sexual preoccupation, and earlier sexual experimentation have been correlated with more frequent consumption of pornography…. Nevertheless, consistent findings have emerged linking adolescent use of pornography that depicts violence with increased degrees of sexually aggressive behavior. The literature does indicate some correlation between adolescents’ use of pornography and self-concept. Girls report feeling physically inferior to the women they view in pornographic material, while boys fear they may not be as virile or able to perform as the men in these media. Adolescents also report that their use of pornography decreased as their self-confidence and social development increase. Additionally, research suggests that adolescents who use pornography, especially that found on the Internet, have lower degrees of social integration, increases in conduct problems, higher levels of delinquent behavior, higher incidence of depressive symptoms, and decreased emotional bonding with caregivers.
3) “difficulty regulating urges”
The claim that no study has reported “difficultly regulating urges” is as untrue as the preceding claim concerning negative effects. The many porn and sex addiction questionnaires listed under #2 assessed whether subjects had trouble controlling their porn use or sexual behaviors. Once again, “inability to control use, despite negative consequences” is a hallmark of an addiction process – and is assessed by standard questionnaires. We provide a few examples from the above list of porn/sex addiction instruments.
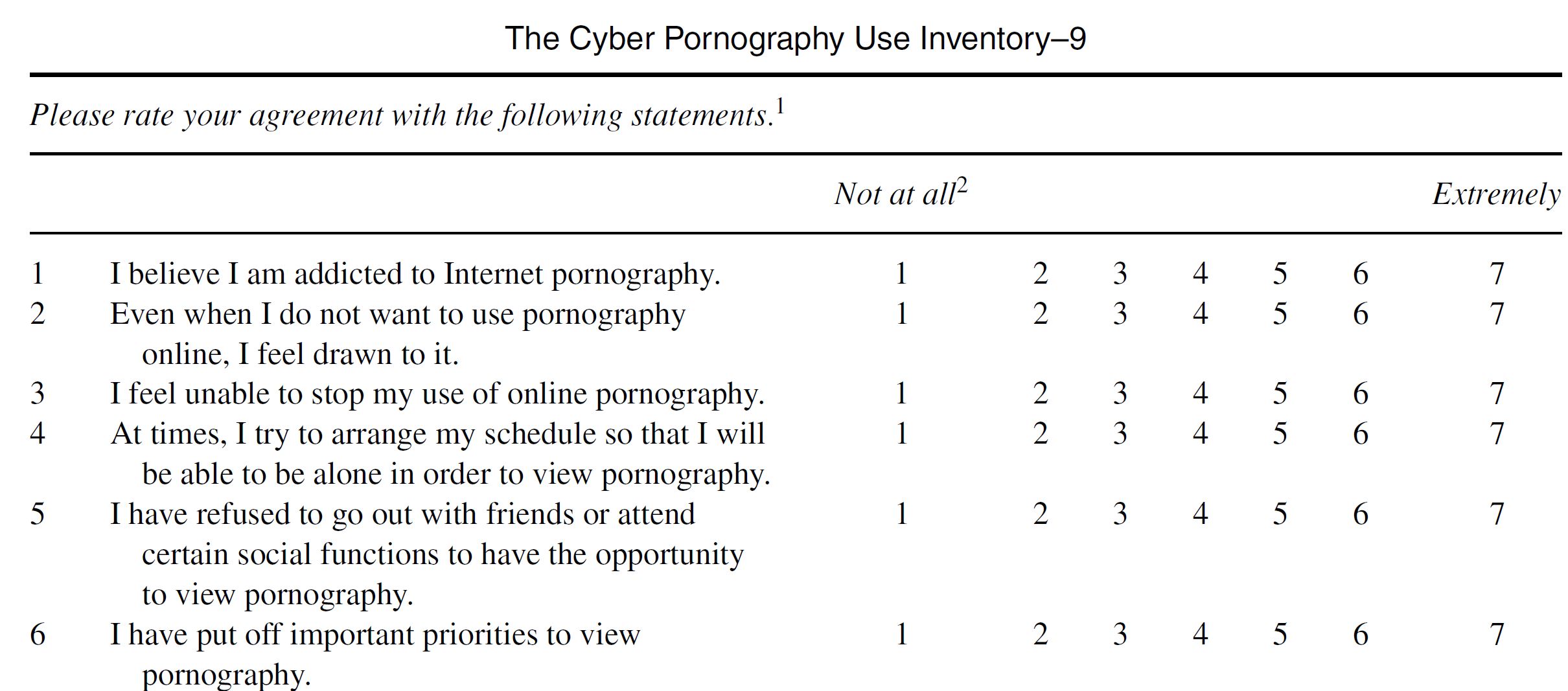
Cyber Pornography Use Inventory (CPUI) –
——————
Problematic Pornography Use Scale (PPUS) –
—————–
Sexual Compulsivity Scale (SCS) –
——————
Hypersexual Behavior Inventory (HBI) –
—————–
No need to fill up this section with CSB questionnaires. You get the idea – Prause et al’s claim that no study has ever reported “inability to control use” is nonsense and an affront to the Lancet journal that published their letter.
4) “reward deficiency syndrome”
As mentioned above “Reward Deficiency Syndrome” (RDS) is not a universally agreed upon element of addiction. Prause et al. tossed RDS into their list to give the false impression that it was a key element addiction that had yet to be reported. Although there is not a scholarly consensus about RDS, it has been assessed (more below).
As conceived by researcher Kenneth Blum, “Reward Deficiency Syndrome” is described as genetically-induced low dopamine signalling, probably arising from a deficiency in dopamine receptors. According to Blum’s hypothesis, RDS manifests as feeling less pleasure (anhedonia) than people with so-called normal dopamine functioning. Moreover, those with RDS with be more likely compensate for low dopamine (less pleasure) by over-consuming natural rewards (junk food, gambling sex) and addictive drugs, and thus run a higher chance of becoming addicts.
I suggest this easy to understand article by Marc Lewis: When the Thrill is Gone: Reward Deficiency Syndrome. Lewis explains the primary problem with the hypotheses:
Despite its appeal, there are some serious problems with the RDS model. I’ll name just two. We know from dozens of studies that drug or alcohol use itself leads to a reduction in dopamine receptor density, or at least dopamine receptor activation, because those receptors tend to burn out or become desensitized when we keep bombarding them with fun stuff.
In other words, RDS isn’t always genetic, as it can be caused by the addiction process itself. When addiction causes lower dopamine signaling, or a decline in reward sensitivity, its called desensitization. As explained earlier, desensitization leads to tolerance, which is a need for greater an greater stimulation to achieve the same high or arousal state. Contrary to Prause’s vague assertions about RDS, six neuroscience-based studies have reported findings consistent with desensitization or habituation: 1, 2, 3, 4, 5, 6, 7, 8. If we also consider the many habituation and escalation studies listed above, 40 more arguably fall under “desensitization” or “decreased reward sensitivity.”.
The prevailing theory of addiction – the incentive-sensitization model and the evidence supporting it – were completely ignored by Prause et al. The neurological changes caused by sensitization manifest as increased “wanting” or craving while liking or pleasure diminishes. As Potenza et al pointed out, many CSB studies have reported findings consistent with the incentive sensitization model:
Research into the neurobiology of compulsive sexual behaviour disorder has generated findings relating to attentional biases, incentive salience attributions, and brain-based cue reactivity that suggest substantial similarities with addictions.
All the above can be considered support for the incentive-sensitization model of addiction. The neuroscience-based CSB studies aligning with this model: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22 , 23, 24, 25, 26, 27.
5) “withdrawal syndrome with cessation”
The fact is, withdrawal symptoms are not required to diagnose an addiction. First, you will find the language “neither tolerance nor withdrawal is necessary or sufficient for a diagnosis…” in both the DSM-IV-TR and DSM-5. Second, the oft-repeated sexology claim that “real” addictions cause severe, life-threatening withdrawal symptoms mistakenly conflates physiological dependence with addiction-related brain changes. An excerpt from this 2015 review of literature provides a technical explanation (Neuroscience of Internet Pornography Addiction: A Review and Update):
A key point of this stage is that withdrawal is not about the physiological effects from a specific substance. Rather, this model measures withdrawal via a negative affect resulting from the above process. Aversive emotions such as anxiety, depression, dysphoria, and irritability are indicators of withdrawal in this model of addiction [43,45]. Researchers opposed to the idea of behaviors being addictive often overlook or misunderstand this critical distinction, confusing withdrawal with detoxification [46,47].
In claiming that withdrawal symptoms must be present to diagnosis an addiction Prause et al. makes the rookie mistake of confusing physical dependency with addiction. These terms are not synonymous (Pfaus made this same error in a 2016 article that YBOP critiqued: YBOP response to Jim Pfaus’s “Trust a scientist: sex addiction is a myth” January, 2016)
That said, internet porn research and numerous self-reports demonstrate that some porn users experience withdrawal and/or tolerance – which are also often characteristic of physical dependency. In fact, ex-porn users regularly report surprisingly severe withdrawal symptoms, which are reminiscent of drug withdrawals: insomnia, anxiety, irritability, mood swings, headaches, restlessness, poor concentration, fatigue, depression, and social paralysis, as well as the sudden loss of libido that guys call the ‘flatline’ (apparently unique to porn withdrawal). Another sign of physical dependency reported by porn users is inability to get an erection or to have an orgasm without using porn.
As for studies, only four have directly asked porn users/sex addicts about withdrawal symptoms. All 4 reported withdrawal symptoms: 1, 2, 3. 4. Three of the studies are described below.
First let’s reconsider the study described in the tolerance/escalation section above, the goal of which was to develop and test a problematic porn use questionnaire. Note that substantial evidence of both “tolerance” and “withdrawal” was found in at-risk users and low-risk users.

Second, a 2018 paper reported on The Development and Validation of the Bergen-Yale Sex Addiction Scale With a Large National Sample. It also assessed withdrawal and tolerance. The most prevalent “sex addiction” components seen in the subjects were salience/craving and tolerance, but the other components, including withdrawal, also showed up.
Cited above – Prevalence, Patterns and Self-Perceived Effects of Pornography Consumption in Polish University Students: A Cross-Sectional Study (2019). The study reported everything Prause claims doesn’t exist: tolerance/habituation, escalation of use, needing more extreme genres to be sexually aroused, withdrawal symptoms when quitting, porn-induced sexual problems, porn addiction, and more. A few excerpts related to tolerance/habituation/escalation:
The study reported withdrawal symptoms upon cessation, even in non-addicts (a definitive sign of addiction-related brain changes):
Among those surveyed who declared themselves to be current pornography consumers (n = 4260), 51.0% admitted to making at least one attempt to give up using it with no dif ference in the frequency of these attempts between males and females. 72.2% of those attempting to quit pornography use indicated the experience of at least one associated e ffect, and the most frequently observed included erotic dreams (53.5%), irritability (26.4%), attention disturbance (26.0%), and sense of loneliness (22.2%) (Table 2).
Additional studies reporting evidence of withdrawal or tolerance are collected here.
6) “enhanced late positive potentials”
The reason Prause’s Lancet letter listed “enhanced late positive potentials” is because she and her team had found lower late positive potentials in her 2015 study – Prause et al., 2015.
EEGs measure electrical activity, or brain waves, on the scalp. “Enhanced late positive potentials” are EEG readings measured immediately after an image seen by the subject. This is but one of many spikes in electrical activity assessed by an EEG, and very much up for interpretation.
What is agreed upon is that lower EEG readings in Prause’s frequent porn users meant they paid less attention to the photos of vanilla porn than the subjects who used less porn. The former were simply bored. Undeterred, Prause boldly claimed “This pattern appears different from substance addiction models.”
But Prause’s finding of lower brain activation for the more frequent porn users actually aligns with the addiction model: it indicates desensitization (habituation) and tolerance, which is the need for greater stimulation to achieve arousal. Nine peer-reviewed papers agree that Prause et al., 2015 actually found desensitization/habituation (a sign of addiction):
- Neuroscience of Internet Pornography Addiction: A Review and Update (2015)
- Decreased LPP for sexual images in problematic pornography users may be consistent with addiction models. Everything depends on the model (Commentary on Prause et al., 2015)
- Neurobiology of Compulsive Sexual Behavior: Emerging Science (2016)
- Should compulsive sexual behavior be considered an addiction? (2016)
- Is Internet Pornography Causing Sexual Dysfunctions? A Review with Clinical Reports (2016)
- Conscious and Non-Conscious Measures of Emotion: Do They Vary with Frequency of Pornography Use? (2017)
- Neurocognitive mechanisms in compulsive sexual behavior disorder (2018)
- Online Porn Addiction: What We Know and What We Don’t—A Systematic Review (2019)
- The Initiation and Development of Cybersex Addiction: Individual Vulnerability, Reinforcement Mechanism and Neural Mechanism (2019)
Even if Prause were correct that her subjects had less “cue-reactivity,” rather than habituation, she conveniently ignores the gaping hole in her “falsification” assertion: 26 other neurological studies have reported cue-reactivity or cravings (incentive sensitization) in compulsive porn users: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22 , 23, 24, 25, 26, 27.
Scientific consensus doesn’t rest on someone’s claims about a lone anomalous study hampered by serious methodological flaws; scientific consensus rests on the preponderance of evidence (unless you are agenda-driven).
Responding to the Prause et al., 2017 “glutamate transmission” red herring
PRAUSE ET AL: A key neurobiological feature of addiction is the increased responsiveness of glutamate neurons that synapse on the nucleus accumbens. These changes might affect long-term sensitisation of the mesocorticolimbic dopamine pathway, as manifested by a range of symptoms including cue-induced craving and compulsive drug use. 3 To date, research on the effects of sex on glutamate function and its modulation of dopamine pathways is scarce.
Why was this included in the Prause letter? Decades of animal research have molded the prevailing theory of addiction: the incentive-sensitization model of addiction. The central brain change behind the theory is as described above – long-term sensitization of the mesocorticolimbic dopamine via glutamate neurons. That’s quite a mouthful, but YBOP wrote a relatively simple article about it in 2011 (with a few pictures): Why Do I Find Porn More Exciting Than A Partner? (2011).
In simple terms, thoughts, feelings, and memories from all over the brain are sent to the brain’s reward system via glutamate-releasing pathways. With addiction, these glutamate pathways become super-powerful, or sensitized. These sensitized pathways can be thought of as Pavlovian conditioning on turbos. When activated by thoughts or triggers, sensitized pathways blast the reward circuit, firing up hard-to-ignore cravings.
But here’s the deal. There are already 24 neuroscience-based studies reporting brain activation patterns and cue-induced cravings definitively demonstrating sensitization in CSB subjects and porn users: 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25.
We don’t need “glutamate studies”, which have only been recently done in human subjects, and are very expensive and challenging to interpret.
Responding to Prause et al., 2017 “supraphysiological stimulation” red herring
PRAUSE ET AL: Sex is a primary reward, with unique peripheral representation. Engagement in sex is positively associated with health and life satisfaction. Sex does not allow for supraphysiological stimulation.
Prause presents us with two red herrings having nothing to do with the debate surrounding compulsive sexual behavior disorder.
Red herring #1: “Engagement in sex is positively associated with health and life satisfaction“.
While engaging in sexual intercourse is often correlated with better health indices, this has nothing to with porn use, porn addiction, sex addiction, or engaging in other types of sexual activities (the term “sex” is vague, non-scientific, and shouldn’t be used as a catch-all in an academic journal).
First, many of the so-called health benefits claimed to be associated with orgasm, masturbation or “sex” are in fact associated with close contact with another human being, not necessarily with orgasm, and not with masturbation. More specifically, claimed correlations between a few isolated health indicators and sexual intercourse are probably just correlations arising from healthier populations who naturally engage in more sex and masturbation. They are not causal.
Specifically, this review of literature (The Relative Health Benefits of Different Sexual Activities, 2010) found that sexual intercourse was related to positive effects, while masturbation was not. In some cases masturbation was negatively related to health benefits – meaning that more masturbation correlated with poorer health indicators. The conclusion of the review:
“Based upon a broad range of methods, samples, and measures, the research findings are remarkably consistent in demonstrating that one sexual activity (Penile-Vaginal Intercourse and the orgasmic response to it) is associated with, and in some cases, causes processes associated with better psychological and physical functioning.”
“Other sexual behaviors (including when Penile-Vaginal Intercourse is impaired, as with condoms or distraction away from the penile–vaginal sensations) are unassociated, or in some cases (such as masturbation and anal intercourse) inversely associated with better psychological and physical functioning.”
“Sexual medicine, sex education, sex therapy, and sex research should disseminate details of the health benefits of specifically Penile-Vaginal Intercourse, and also become much more specific in their respective assessment and intervention practices.”
Second, Prause is saying that sex addiction cannot exist because “sex” can have positive effects. This is analogous to saying that eating junk food causes no problems because eating food prevents malnourishment and death. The documented health effects of overconsumption of today’s high fat/sugar foods say otherwise. As does the fact that 39% of adult Americans are obese and 75% or more are overweight. Moreover, hundreds of human and animal studies support the assertion that overconsumption of junk food can can alter the brain in ways similar to addictive drugs.
Red herring #2: “Sex does not allow for supraphysiological stimulation“.
Only a handful of people would know that Prause et al. is attempting to discredit the concept of internet pornography as a supernormal stimulus. As its co-authors misuse the term “supraphysiological stimulation,” it’s clear that they have no idea what Nobel laureate Nikolaas Tinbergen meant when he coined the term ‘supernormal stimulus’ (or supranormal).
First, supraphysiological levels of neurotransmitters, such as dopamine or endogenous opioids, are not required for chronic use to induce addiction-related brain changes. For example, the two most addictive drugs (meaning those which hook the greatest percentage of users) – nicotine and opiates – increase reward center dopamine by 200%. This is same levels of dopamine seen in sexual arousal (sex and orgasm produce the highest levels of dopamine and endogenous opioids naturally available).
Moreover, sexual arousal and addictive drugs activate the exact same reward circuit nerve cells. In contrast, there’s only a small percentage of nerve-cell activation-overlap between addictive drugs and other natural rewards such as food or water. The fact that meth, cocaine, and heroin turn on the same nerve cells that make sexual stimulation so compelling helps explain why they can be so addictive.
Research reveals that “supraphysiological stimulation” is not required for addiction. Mountains of research reveal that behavioral addictions (food addiction, pathological gambling, video gaming, Internet addiction and porn addiction) and substance addictions share many of the same fundamental mechanisms leading to a collection of shared alterations in brain anatomy and chemistry.
Finally we have the obvious: both the DSM5 and the ICD-11 recognize behavioral addictions. The DSM5 (2013) contains a diagnosis for gambling addiction, while the new ICD-11 (2018) has diagnoses for gambling addiction as well as video-game addiction, and contains a diagnosis suitable for porn addiction or sex addiction: “Compulsive Sexual Behavior Disorder.”
Second, the authors of Prause et al. have no idea what is meant by supernormal stimulus (mistakenly calling it “supraphysiological stimulation”). For a better understanding, I suggest this short article by a Harvard professor, or this very popular illustrated explanation by Stuart McMillen. Maybe Prause and company could crack open a book, such as Supernormal Stimuli: How Primal Urges Overran Their Evolutionary Purpose by Deirdre Barrett. An excerpt from the book’s 2010 press release:
We now have access to a glut of larger-than-life temptations, from candy to pornography to atomic bombs, which cater to outmoded but persistent instinctive drives with dangerous results. In the 1930s Dutch Nobel laureate Niko Tinbergen found that birds that lay small, pale blue eggs speckled with grey preferred to sit on giant, bright blue plaster dummies with black polka dots. A male silver washed fritillary butterfly was more sexually aroused by a butterfly-sized rotating cylinder with horizontal brown stripes than it is by a real, live female of its own kind. Mother birds preferred to try feeding a fake baby bird beak held on a stick by Tinbergen’s students if the dummy beak was wider and redder than a real chick’s. Male stickleback fish ignored a real male to fight a dummy if its underside was brighter red than any natural fish. Tinbergen coined the term “supernormal stimuli” to describe these imitations, which appeal to primitive instincts and, oddly, exert a stronger attraction than real things. Animals encounter supernormal stimuli mostly when experimenters build them. We humans can produce our own: super sugary drinks, French fries, huge-eyed stuffed animals, diatribes about menacing enemies.
A supernormal stimulus is not defined as supra-physiological response. Rather, it is based upon a comparison between what an animal evolved to find compelling and an exaggerated (perhaps synthetic) version of that same compelling stimulus. Female birds, for example, struggled to sit on Tinbergen’s larger-than life, vividly spotted plaster eggs while their own pale, dappled eggs perished untended.
Internet porn is considered a supernormal stimulus because it provides endless sexual novelty. With internet porn, it’s not just the unending sexual novelty that buzzes our reward system. The reward system fires up for other emotions and stimuli too, all of which often feature prominently in viewers:
- Strong emotions – such as guilt, disgust, embarrassment, anxiety & fear
- Seeking and searching – the reward circuit is often called the seeking circuit
- Anything that violates expectations – shock, surprise, or more than we could have imagined
Erotic words and pictures have been around a long time. So has the neurochemical rush from novel mates. Yet the novelty of a once-a-month Playboy evaporates as soon as you turn the pages. Would anyone call Playboy or softcore videos “shocking” or “anxiety-producing?” Would either violate the expectations of a computer-literate boy over the age of 12? Neither compares with the “searching and seeking” of a multiple-tab Google porn prowl. What makes internet porn unique is that you can keep your dopamine (and sexual arousal) jacked up with the click of a mouse or tap on a screen.
Many of these same emotional states (anxiety, shame, shock, surprise) not only elevate dopamine, but each can also boost stress hormones and neurotransmitters (norepinephrine, epinephrine, cortisol). These stress neurochemicals increase excitement while amplifying dopamine’s already powerful effects. Other qualities that set internet porn apart from other potentially addictive substances and behaviors:
- Studies reveal that video porn is more arousing than static porn.
- To increase sexual arousal (and raise declining dopamine) one can instantly switch genres during a masturbation session. Couldn’t do that before 2006 and the arrival of streaming tube sites.
- Unlike photos of naked people, videos replace your imagination, and may shape your sexual tastes, behavior, or trajectory (especially so for adolescents).
- Porn is stored in your brain, which allows you to recall it anytime you need a “hit.”
- Unlike food and drugs, for which there is a limit to consumption, there are no physical limitations to internet porn consumption. The brain’s natural satiation mechanisms are not activated, unless one climaxes. Even then, the user can click to something more exciting to become aroused again.
- With food and drugs one can only escalate (a marker of an addiction process) by consuming more. With internet porn one can escalate both with more novel “partners” and by viewing new and unusual genres. It’s quite common for a porn user to move to evermore extreme porn. A user can also escalate by viewing compilation videos or by using VR porn.
Highly palatable foods (concentrated sugars/fats/salt), video games, and internet porn are recognized as supernormal stimuli. Here are a few peer-reviewed papers exploring internet applications (porn, video games, Facebook) as supernormal stimuli:
1) Neuroscience of Internet Pornography Addiction: A Review and Update (2015) – Excerpt:
Some internet activities, because of their power to deliver unending stimulation (and activation of the reward system), are thought to constitute supernormal stimuli [24], which helps to explain why users whose brains manifest addiction-related changes get caught in their pathological pursuit. Nobel Prize winning scientist Nikolaas Tinbergen [25] posited the idea of “supernormal stimuli,” a phenomenon wherein artificial stimuli can be created that will override an evolutionarily developed genetic response. To illustrate this phenomenon, Tinbergen created artificial bird eggs that were larger and more colorful than actual bird eggs. Surprisingly, the mother birds chose to sit on the more vibrant artificial eggs and abandon their own naturally laid eggs. Similarly, Tinbergen created artificial butterflies with larger and more colorful wings, and male butterflies repeatedly tried to mate with these artificial butterflies in lieu of actual female butterflies. Evolutionary Psychologist Dierdre Barrett took up this concept in her recent book Supernormal Stimuli: How Primal Urges Overran Their Evolutionary Purpose [26]. “Animals encounter supernormal stimuli mostly when experimenters build them. We humans can produce our own.” [4] (p. 4). Barrett’s examples range from candy to pornography and highly salted or unnaturally sweetened junk food to highly engaging interactive video game playing. In short, generalized internet chronic overuse is highly stimulating. It recruits our natural reward system, but potentially activates it at higher levels than the levels of activation our ancestors typically encountered as our brains evolved, making it liable to switch into an addictive mode [27].
2) Measuring Preference for Supernormal Over Natural Rewards: A Two-Dimensional Anticipatory Pleasure Scale (2015) – Excerpt:
Supernormal (SN) stimuli are artificial products that activate reward pathways and approach behavior more so than naturally occurring stimuli for which these systems were intended. Many modern consumer products (e.g., snack foods, alcohol, and pornography) appear to incorporate SN features, leading to excessive consumption, in preference to naturally occurring alternatives. No measure currently exists for the self-report assessment of individual differences or changes in susceptibility to such stimuli. Therefore, an anticipatory pleasure scale was modified to include items that represented both SN and natural (N) classes of rewarding stimuli. Exploratory factor analysis yielded a two-factor solution, and as predicted, N and SN items reliably loaded on separate dimensions. Internal reliability for the two scales was high, ρ =.93 and ρ =.90, respectively. The two-dimensional measure was evaluated via regression using the N and SN scale means as predictors and self-reports of daily consumption of 21 products with SN features as outcomes. As expected, SN pleasure ratings were related to higher SN product consumption, while N pleasure ratings had either negative or neutral associations to consumption of these products. We conclude that the resulting two-dimensional measure is a potentially reliable and valid self-report measure of differential preference for SN stimuli. While further evaluation is needed (e.g., using experimental measures), the proposed scale may play a useful role in the study of both trait- and state-based variation in human susceptibility to SN stimuli.
Processed foods, psychoactive substances, some retail goods, and various social media and gaming products are readily overconsumed, presenting numerous population health challenges (Roberts, van Vught, & Dunbar, 2012). Evolutionary psychology provides a persuasive explanation of excessive consumption. Animals, including humans, tend to approach (i.e., gather, acquire, and consume) stimuli that provide the highest relative reward for their efforts, thereby optimizing their utility (Chakravarthy & Booth, 2004; Kacelnik & Bateson, 1996). Neurological reward mechanisms evolved to promote adaptive behavior by reinforcing stimuli that send signals of promoting fitness, such as providing nutrients or reproductive opportunities. Tinbergen (1948) coined the term “Supernormal Stimulus” upon finding that animals tend to exhibit heightened responses to exaggerated versions of natural stimuli. This “selection asymmetry” (Staddon, 1975; Ward, 2013) is not maladaptive in natural environments in which exaggerated versions of the stimulus are rare—but presents problems when artificial and exaggerated alternatives exist. For example, the newly hatched herring gull prefers to peck at a fabricated thin red rod with white bands at its tip, rather than its mother’s naturally red spotted thin beak (Tinbergen & Perdeck, 1951). In the context of resource selection, the outcome is a behavioral heuristic of “get all you can”: an adaptive strategy in natural environments where resource supply is scarce or unreliable. In the modern human environment, many highly rewarding experiences exist in the form of artificial consumer products that have been designed or refined to be supernormal. That is, they stimulate an evolved reward system to a degree not found in natural stimuli (Barrett, 2010). For example, psychoactive substances (Nesse & Berridge, 1997), commercial fast-food products (Barrett, 2007), gambling products (Rockloff, 2014), television shows (Barrett, 2010; Derrick, Gabriel, & Hugenberg, 2009), digital social networking and the Internet (Rocci, 2013; Ward, 2013), and various retail products, such as expensive cars (Erk, Spitzer, Wunderlich, Galley, & Walter, 2002), high-heeled shoes (Morris, White, Morrison, & Fisher, 2013), cosmetics (Etcoff, Stock, Haley, Vickery, & House, 2011), and children’s toys (Morris, Reddy, & Bunting, 1995) have all been discussed as forms of modern day supernormal stimuli. For some of these stimuli, neurological evidence has shown that they tend to activate dopamine pathways intensely, hijacking the reward response designed for natural rewards, thereby promoting excess consumption and in some cases, addiction (Barrett, 2010; Blumenthal & Gold, 2010; Wang et al., 2001).
To varying degrees, supernormal stimuli tend to be unhealthy. The ready availability of high-calorie takeaway meals and snacks, the toxicity of alcohol and other substances, the sedentary activity involved in watching television, using digital media and gaming products, and the expense of retail items or gambling, all serve to provide an environment that fosters unhealthy behavioral choices, leading to harms (Barrett, 2007, 2010; Birch, 1999; Hantula, 2003; Ward, 2013). This makes the study of susceptibility of modern humans to supernormal stimuli of practical significance. In the current report, we use the term supernormal stimuli to refer to modern human products and experiences that are characterized by asymmetric selectivity (uncontrolled approach to more intense variants) and being made artificially abundant in the modern world. These products are often processed, refined, or synthesized consumer goods including snack foods or substances. Less obvious examples include messages received via social media. Although at times less stimulating than a face-to-face conversation, this communication method provides prolonged enhanced visual, speed, and delivery characteristics. Similarly, most modern day clothing and other retail products exhibit similar enhanced signifiers of rarity or desirability, with attendant implications for sexual or social status. Consumption or acquisition of these products is theorized to provide immediate reward due to being interpreted as fitness enhancing.
It has been suggested a preference for supernormal reward could be the result of differences in dopamine functioning. Dopamine deficiency has been found to be related to various forms of excess consumption including alcohol abuse, binge eating, problem gambling, and Internet addiction (Bergh, Eklund, Södersten, & Nordin, 1997; Blum, Cull, Braverman, & Comings, 1996; Johnson & Kenny, 2010; Kim et al., 2011). The concept of supernormal susceptibility is consistent with an interpretation in terms of individual variability in the dopamine functioning. Dopaminergic pathways, evolved to prioritize resource acquisition and consumption in a resource-scarce environment, are likely to be particularly sensitive to psychoactive substances, energy-dense food, and other modern day consumer products exhibiting exaggerated reward properties (Barrett, 2010; Nesse & Berridge, 1997; Wang et al., 2001). If this is the case, then the two-dimensional NPS/SNPS described here would be expected to discriminate individuals with dopamine dysfunction. Future research might profitably employ neurophysiological techniques in conjunction with self-report measures, in order to confirm the correspondences between these two levels of description.
Supernormal experiences are inherently unhealthy and amenable to excess consumption due to their processed characteristics (e.g., snacks and take away foods) and encouraging prolonged sedentary behavior (e.g., social networking and gaming). Therefore, the ability to identify individuals who prefer these types of reward provides a valuable contribution to those researching, treating, and preventing population health problems caused by over consumption.
3) Pornography addiction – a supranormal stimulus considered in the context of neuroplasticity (2013) – Excerpt:
Addiction has been a divisive term when applied to various compulsive sexual behaviors (CSBs), including obsessive use of pornography. Despite a growing acceptance of the existence of natural or process addictions based on an increased understanding of the function of the mesolimbic dopaminergic reward systems, there has been a reticence to label CSBs as potentially addictive. While pathological gambling (PG) and obesity have received greater attention in functional and behavioral studies, evidence increasingly supports the description of CSBs as an addiction. This evidence is multifaceted and is based on an evolving understanding of the role of the neuronal receptor in addiction-related neuroplasticity, supported by the historical behavioral perspective. This addictive effect may be amplified by the accelerated novelty and the ‘supranormal stimulus’ (a phrase coined by Nikolaas Tinbergen) factor afforded by Internet pornography….
It is surprising that food addiction would not be included as a behavioral addiction, despite studies demonstrating dopaminergic receptor downregulation in obesity (Wang et al., 2001), with reversibility seen with dieting and normalization of body mass index (BMI) (Steele et al., 2010). The concept of a ‘supranormal stimulus’, invoking Nikolaas Tinbergen’s term (Tinbergen, 1951), has recently been described in the context of intense sweetness surpassing cocaine reward, which also supports the premise of food addiction (Lenoir, Serre, Laurine, & Ahmed, 2007). Tinbergen originally found that birds, butterflies, and other animals could be duped into preferring artificial substitutes designed specifically to appear more attractive than the animal’s normal eggs and mates. There is, of course, a lack of comparable functional and behavioral work in the study of human sexual addiction, as compared to gambling and food addictions, but it can be argued that each of these behaviors can involve supranormal stimuli. Deirdre Barrett (2010) has included pornography as an example of a supranormal stimulus…..
Pornography is a perfect laboratory for this kind of novel learning fused with a powerful pleasure incentive drive. The focused searching and clicking, looking for the perfect masturbatory subject, is an exercise in neuroplastic learning. Indeed, it is illustrative of Tinbergen’s concept of the ‘supranormal stimulus’ (Tinbergen, 1951), with plastic surgery–enhanced breasts presented in limitless novelty in humans serving the same purpose as Tinbergen’s and Magnus’s artificially enhanced female butterfly models; the males of each species prefer the artificial to the naturally evolved (Magnus, 1958; Tinbergen, 1951). In this sense, the enhanced novelty provides, metaphorically speaking, a pheromone-like effect in human males, like moths, which is ‘inhibiting orientation’ and ‘disrupting pre-mating communication between the sexes by permeating the atmosphere’ (Gaston, Shorey, & Saario, 1967)…..
Even public opinion seems to be trying to describe this biologic phenomenon, as in this statement from Naomi Wolf; ‘For the first time in human history, the images’ power and allure have supplanted that of real naked women. Today real naked women are just bad porn’ (Wolf, 2003). Just as Tinbergen’s and Magnus’s ‘butterfly porn’ successfully competed for male attention at the expense of real females (Magnus, 1958; Tinbergen, 1951), we see this same process occurring in humans.
4) Is Internet Pornography Causing Sexual Dysfunctions? A Review with Clinical Reports (2016) – Excerpt:
3.2. Internet Pornography as Supernormal Stimulus
Arguably, the most important development in the field of problematic sexual behavior is the way in which the Internet is influencing and facilitating compulsive sexual behavior [73]. Unlimited high-definition sexual videos streaming via “tube sites” are now free and widely accessible, 24 h a day via computers, tablets and smartphones, and it has been suggested that Internet pornography constitutes a supernormal stimulus, an exaggerated imitation of something our brains evolved to pursue because of its evolutionary salience [74,75]. Sexually explicit material has been around for a long time, but (1) video pornography is significantly more sexually arousing than other forms of pornography [76,77] or fantasy [78]; (2) novel sexual visuals have been shown to trigger greater arousal, faster ejaculation, and more semen and erection activity compared with familiar material, perhaps because attention to potential novel mates and arousal served reproductive fitness [75,79,80,81,82,83,84]; and (3) the ability to self-select material with ease makes Internet pornography more arousing than pre-selected collections [79]. A pornography user can maintain or heighten sexual arousal by instantly clicking to a novel scene, new video or never encountered genre. A 2015 study assessing Internet pornography’s effects on delay discounting (choosing immediate gratification over delayed rewards of greater value) states, “The constant novelty and primacy of sexual stimuli as particularly strong natural rewards make internet pornography a unique activator of the brain’s reward system. … It is therefore important to treat pornography as a unique stimulus in reward, impulsivity, and addiction studies” [75] (pp. 1, 10).
Novelty registers as salient, enhances reward value, and has lasting effects on motivation, learning and memory [85]. Like sexual motivation and the rewarding properties of sexual interaction, novelty is compelling because it triggers bursts of dopamine in regions of the brain strongly associated with reward and goal-directed behavior [66]. While compulsive Internet pornography users show stronger preference for novel sexual images than healthy controls, their dACC (dorsal anterior cingulate cortex) also shows more rapid habituation to images than healthy controls [86], fueling the search for more novel sexual images. As co-author Voon explained about her team’s 2015 study on novelty and habituation in compulsive Internet pornography users, “The seemingly endless supply of novel sexual images available online [can feed an] addiction, making it more and more difficult to escape” [87]. Mesolimbic dopamine activity can also be enhanced by additional properties often associated with Internet pornography use such as, violation of expectations, anticipation of reward, and the act of seeking/surfing (as for Internet pornography) [88,89,90,91,92,93]. Anxiety, which has been shown to increase sexual arousal [89,94], may also accompany Internet pornography use. In short, Internet pornography offers all of these qualities, which register as salient, stimulate dopamine bursts, and enhance sexual arousal.
Prause et al., 2017 doesn’t understand the addiction model
PRAUSE ET AL: Also, data are not sufficient to differentiate between compulsive and impulsive models.
Another red herring. Unlike the authors of Potenza et al., the authors of Prause et al., are not addiction experts – and it shows. Studies repeatedly report that addiction features elements of both impulsivity and compulsivity. (A Google Scholar search for addiction + impulsivity + compulsivity returns 22,000 citations.) Here are simple definitions of impulsivity and compulsivity:
- Impulsivity: Acting quickly and without adequate thought or planning in response to internal or external stimuli. A predisposition to accept smaller immediate rewards over larger delayed gratification and an inability to stop a behavior toward gratification once it’s set in motion.
- Compulsivity: Refers to repetitive behaviors that are performed according to certain rules or in a stereotypical fashion. These behaviors persevere even in the face of adverse consequences.
Predictably, addiction researchers often characterize addiction as developing from impulsive pleasure-seeking behavior to compulsive repetitive behaviors to avoid discomfort (such as the pain of withdrawal). Thus, addiction comprises a bit of both, along with other elements. So the distinctions between “models” of impulsivity and compulsivity as they relate to CSBD are somewhat artificial.
The use of “compulsive” in the new ICD-11 diagnosis isn’t meant to denote the neurological underpinnings of Compulsive Sexual Behavior Disorder: “continued repetitive sexual behaviour despite adverse consequences.” Instead “compulsive,” as used in the ICD-11, is a descriptive term that has been in use for years, and is often employed interchangeably with “addiction.” (For example a Google scholar search for compulsion + addiction returns 130,000 citations.)
Thus, whatever you or your healthcare giver want to call it – “hypersexuality,” “porn addiction,” “sex addiction,” “out-of-control sexual behavior,” “cybersex addiction” – if the behaviors fall within the “Compulsive Sexual Behaviour Disorder” description, the condition can be diagnosed using the ICD-11 CSBD diagnosis.